High cholesterol and high blood pressure often show up together, and both conditions damage the same blood vessels, through the same biological pathways, at the same time. The American Heart Association updated its blood pressure guideline in 2025, the first change since 2017, and a new 2026 cholesterol guideline from the American College of Cardiology now treats these two conditions as a linked pair rather than separate problems.
Doctors call this combination one of the strongest predictors of heart attack and stroke. This guide breaks down why high cholesterol and high blood pressure feed off each other, what happens inside your arteries when both are present, and which changes actually move the needle on both numbers at once.
The Connection Between High Cholesterol and Hypertension
High cholesterol and high blood pressure damage the same vessel lining, through overlapping mechanisms, and that overlap is why one condition speeds up the other. The connection between high cholesterol and hypertension comes down to your arteries. When cholesterol builds plaque and pressure pounds against vessel walls, you get a feedback loop that gets worse on its own unless something interrupts it.
How Cholesterol Affects Blood Vessels
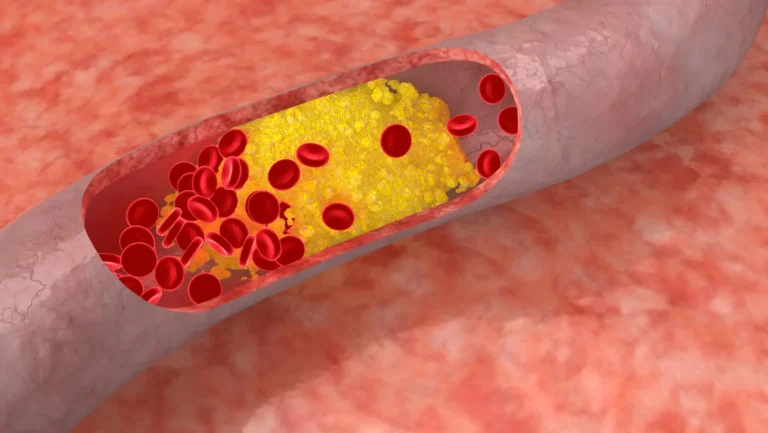
Cholesterol travels through your blood packed inside particles called lipoproteins. LDL, the “bad” type, slips into the artery wall when the lining gets damaged or leaky. Once inside, LDL gets oxidized by free radicals. Your immune system sends white blood cells to clean up the mess, but those cells get stuck, swell up with fat, and turn into foam cells.
Foam cells pile up and form fatty streaks. Over the years, those streaks harden into plaque. This whole process is called atherosclerosis, and it’s the foundation for most heart attacks and strokes.
How Hypertension Develops
Blood pressure measures the force your blood applies to artery walls as your heart pumps. Several things push that force higher: arteries that have lost their natural flexibility, kidneys that hold onto too much sodium, blood vessels that stay too narrow, and a nervous system stuck in overdrive.
Diet, body weight, alcohol, and stress pull the trigger. Most cases of high blood pressure, around 90 to 95 percent, have no single identifiable cause and get labeled “primary hypertension.”
Shared Risk Factors
The same habits and traits raise both numbers:
- Diets high in sodium, refined carbs, and trans fats
- Carrying extra weight, especially around the abdomen
- Sitting most of the day
- Smoking
- Drinking more than one or two alcoholic drinks daily
- Chronic stress and poor sleep
- A family history of either condition
- Getting older, since both arteries and blood pressure regulation change with age
If you have one of these risk factors, check your cholesterol and your blood pressure at the same visit, since high cholesterol and high blood pressure tend to move together.
What Happens Inside Your Arteries When Both High Cholesterol and High Blood Pressure Are Present?
High cholesterol and high blood pressure actively accelerate each other’s damage through a five-step chain reaction inside the vessel wall. Once you see the sequence, the urgency to treat both conditions together becomes obvious.
Step 1: Damage to the Artery Wall
High blood pressure batters the inner lining of your arteries, called the endothelium, with constant mechanical force. This thin layer is supposed to act like a smooth, selective gatekeeper. Under sustained pressure, gaps open between the cells that make up that lining, and your arteries starts leaking.
Step 2: Cholesterol Infiltration
Once your arteries start leaking, LDL particles flood through far more easily. Research using arterial wall modeling has shown that hypertension physically increases water filtration and particle movement across the vessel wall, meaning higher pressure doesn’t just coincide with more LDL buildup, it mechanically forces more of it inside.
Step 3: Plaque Formation
Trapped LDL oxidizes. White blood cells called monocytes squeeze into the wall to clear it out, transform into foam cells, and start the buildup of plaque that defines high cholesterol and high blood pressure damage at the cellular level.
Smooth muscle cells migrate in too, adding bulk to the growing lesion. A fibrous cap eventually forms over the plaque, sealing it inside the artery wall like a blister under skin.
Step 4: Arterial Narrowing and Stiffening
As plaque thickens, the artery’s interior space shrinks. The vessel wall also loses elasticity because plaque deposits replace the stretchy tissue that normally absorbs the pulse of each heartbeat. Stiffer, narrower arteries force the heart to pump harder, which raises blood pressure further.
Step 5: Increased Cardiovascular Risk
A narrowed, stiffened artery is a setup for two outcomes. Either the plaque keeps growing until it blocks blood flow on its own, or the fibrous cap ruptures and triggers a blood clot that blocks the vessel almost instantly.
The first pattern causes slow, progressive symptoms. The second causes heart attacks and strokes with little warning. This entire chain is why cardiologists no longer treat high cholesterol and high blood pressure as separate line items on a lab report.
Why High Blood Pressure Makes Cholesterol More Dangerous
Pressure makes existing cholesterol behave worse. Mechanical stress from hypertension speeds up how fast LDL oxidizes into the more damaging form that drives plaque growth. Higher pressure also increases wall shear stress at curves and branch points, the exact spots where plaque tends to form first.
A person with LDL of 160 mg/dL and normal blood pressure faces a different risk than someone with the same LDL and stage 2 hypertension. This is the core reason high cholesterol and high blood pressure combined accelerate plaque faster than either condition alone.
Why High Cholesterol Makes High Blood Pressure Harder on the Body
As plaque builds inside artery walls, vessels lose their ability to expand and relax with each heartbeat, a property called vascular compliance. Stiff, narrowed arteries can’t buffer blood flow the way healthy ones do, so existing high blood pressure climbs higher and gets harder to control with the same medications that worked before. Plaque buildup also damages cells responsible for producing nitric oxide, the molecule that signals vessels to relax.
Less nitric oxide means more constriction, and more constriction means higher readings. This is one reason doctors sometimes add a second or third blood pressure medication once plaque has formed, even when hypertension started out mild.
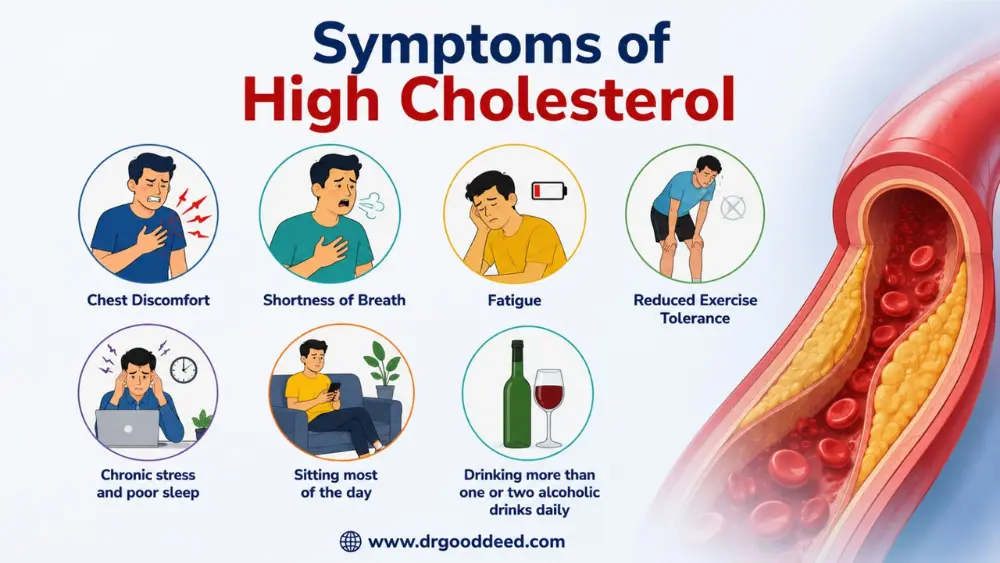
Symptoms of High Cholesterol
Both cholesterol or blood pressure conditions can run for decades without a single symptom while damage builds underneath. Symptoms tend to show up only once a complication has already started.
Potential Warning Signs of Cardiovascular Disease
When symptoms appear, they usually mean the arteries have already narrowed significantly, not that trouble is just beginning. Watch for these patterns instead of waiting for obvious pain.
Chest Discomfort
Pressure or squeezing in the chest, especially during activity or stress, can mean a coronary artery has narrowed enough to limit blood flow to the heart muscle. This is angina, and it often eases with rest. Chest discomfort that doesn’t ease with rest needs emergency care immediately.
Shortness of Breath
Feeling winded during activities that used to feel easy, like climbing one flight of stairs, can point to reduced blood flow to the heart or early heart failure from years of unmanaged blood pressure.
Fatigue and Reduced Exercise Tolerance
A heart working against stiff, narrowed arteries pumps less efficiently. People often describe this as a slow decline rather than a sudden change, which makes it easy to dismiss as normal aging instead of a warning sign.
Complications That May Reveal the Conditions
Sometimes the first sign of high cholesterol and high blood pressure is a complication itself: a heart attack, a stroke, peripheral artery disease causing leg pain while walking, or vision changes from damaged blood vessels in the eyes. This is why routine screening matters more than symptom-watching.
The CDC reports that nearly half of American adults have hypertension, and a large share don’t know it until a routine check or a medical event reveals it.
Which Is More Dangerous: High Cholesterol or High Blood Pressure?
Comparing high cholesterol and high blood pressure as if one wins a danger contest ignores how cardiovascular risk actually works. Risk is a combination of factors stacking on top of each other inside the same arteries.
Four things determine actual danger, regardless of which condition someone wants to rank first:
- Severity: An LDL of 190 mg/dL carries different risk than an LDL of 145 mg/dL. A systolic pressure of 165 mmHg carries different risk than 134 mmHg.
- Duration: Thirty years of mildly elevated cholesterol can cause more plaque than five years of severely elevated cholesterol. Time matters as much as the number itself.
- Other risk factors: Smoking, diabetes, age, family history, and kidney function all multiply risk rather than simply adding to it.
- Presence of both conditions: Someone with both high cholesterol and high blood pressure faces compounded risk that exceeds the sum of either condition alone, because of the feedback loop described earlier.
A 55-year-old with borderline cholesterol and well-controlled blood pressure faces less danger than a 40-year-old with moderate cholesterol and uncontrolled stage 2 hypertension. The honest answer is that asking which condition is “worse” wastes the time that’s better spent managing both.
Strategy That Improves Both High Cholesterol and High Blood Pressure Conditions Simultaneously
Managing high cholesterol and hypertension together works because they share root causes, and fixing the root often improves both lab values without separate interventions for each one.
Focus on Shared Root Causes
Visceral fat, insulin resistance, chronic inflammation, and sodium-heavy diets drive both conditions through overlapping biological pathways. Target these root causes, and cholesterol and blood pressure numbers tend to move in the right direction together rather than one improving while the other stays flat.
The High-Impact Lifestyle Changes (Ranked)
This list is ordered by the size of effect each change produces, based on the consistency of results across clinical research.
1. Improve Dietary Quality
Cut sodium to under 2,300 mg daily, and ideally closer to 1,500 mg if you already have hypertension. Replace saturated fat with sources like olive oil, nuts, and fatty fish. The DASH diet and Mediterranean-style eating patterns are the two approaches with the strongest evidence behind them for lowering cholesterol and blood pressure naturally, because both emphasize vegetables, whole grains, lean protein, and minimal processed food.
2. Increase Physical Activity
Aim for at least 150 minutes of moderate aerobic activity weekly, such as brisk walking, cycling, or swimming. Add two sessions of strength training. Exercise raises HDL, the protective cholesterol type, while directly lowering systolic blood pressure through improved vessel flexibility.
3. Reduce Visceral Fat
The fat stored around your organs, not just under your skin, drives inflammation that worsens both conditions. Losing even 5 to 10 percent of body weight produces measurable improvements in both LDL and blood pressure readings within a few months.
4. Improve Sleep Quality
Poor sleep raises cortisol and disrupts the hormones that regulate blood pressure overnight. Adults who sleep less than six hours regularly show higher rates of both hypertension and unfavorable cholesterol patterns compared to those getting seven to eight hours.
5. Stop Smoking
Smoking damages the endothelium directly, lowers HDL, and stiffens arteries within years. Quitting reverses some of this damage faster than most people expect. Blood pressure can improve within weeks, and HDL levels often rise within a year.
FAQs
Can high cholesterol cause high blood pressure?
Yes. Plaque buildup stiffens artery walls and reduces nitric oxide production, both of which directly raise blood pressure. This effect strengthens over years as plaque accumulates, not immediately after a single high cholesterol reading.
Why do these conditions often occur together?
They share root drivers: visceral fat, insulin resistance, high sodium intake, and chronic inflammation. These factors damage the same arterial lining through overlapping pathways, so one condition’s presence raises the odds of the other.
Can lowering cholesterol help reduce blood pressure?
Yes, modestly. Statin therapy improves endothelial function and arterial flexibility, producing systolic reductions of roughly 2 to 5 mmHg in several clinical trials. It works as a supporting effect, not a primary blood pressure treatment.
How are high cholesterol and hypertension diagnosed?
A fasting or non-fasting lipid panel measures LDL, HDL, and triglycerides. Blood pressure needs two separate readings, on two separate days, averaging 130/80 mmHg or higher to confirm hypertension under current AHA criteria.
What is the best diet for managing both conditions?
The DASH diet, built around vegetables, whole grains, and low sodium, has the strongest trial evidence for lowering both LDL and blood pressure. The Mediterranean diet ranks a close second with similar dual benefits.
What exercises help lower cholesterol and blood pressure?
Brisk walking, cycling, swimming, and other moderate aerobic activities for 150 minutes weekly raise HDL and lower systolic pressure. Add two weekly strength sessions for additional LDL improvement beyond aerobic exercise alone.
Are medications often needed for both problems?
Often, yes, especially once LDL exceeds 160 mg/dL or blood pressure stays at stage 2 levels despite lifestyle changes. Statins and antihypertensives are frequently prescribed together because each drug class supports the other’s effect on arteries.
How can I lower cholesterol and blood pressure naturally?
Cut sodium below 1,500 to 2,300 mg daily, lose 5 to 10 percent of body weight if overweight, and walk 30 minutes most days. Replace saturated fats with olive oil and fish. These changes target shared root causes directly.
Sources
- American Heart Association: 2025 Hypertension Guideline Update
- American College of Cardiology / American Heart Association: 2026 Guideline on the Management of Dyslipidemia
- Centers for Disease Control and Prevention: Facts About Hypertension
- National Heart, Lung, and Blood Institute: Atherosclerosis
- JACC: Role of Endothelial Shear Stress in Coronary Atherosclerosis