

The signs your antidepressant dose is too low include persistent low mood, ongoing fatigue, unresolved anxiety, and poor sleep, all continuing beyond 6 to 8 weeks of use. In the US, studies estimate that up to 50% of patients on antidepressants receive a subtherapeutic dose, meaning a dose that does not reach clinical effectiveness.
This is one of the most overlooked reasons antidepressant treatment fails. This guide covers the specific symptoms, how to tell the difference between a wrong dose and a wrong drug, and what doctors do to fix it.
Symptoms of Underdosed Antidepressants
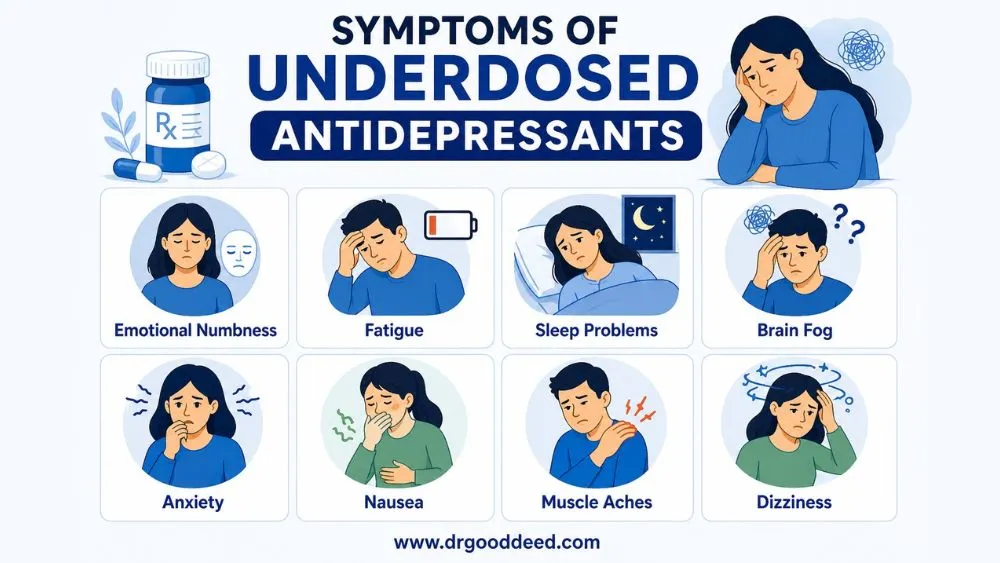
Symptoms of underdosed antidepressants are often misread as treatment failure or the natural course of depression. They are not. They are specific and recognizable. The clinical term is a subtherapeutic response, meaning the drug is present in the body but not at the concentration needed to produce full receptor engagement.
Knowing the signs your antidepressant dose is too low early prevents weeks of unnecessary suffering.
Persistent Low Mood or Emotional Numbness
A correctly dosed antidepressant should produce noticeable mood improvement by week 6 to 8. If low mood, emptiness, or feeling emotionally flat continues beyond that window, the dose needs reassessment. Emotional numbness in particular is a sign that serotonin reuptake inhibition is incomplete, meaning the drug is partially working but not enough.
Low Energy and Fatigue Despite Medication
Fatigue that persists after 4 to 6 weeks on an SSRI or SNRI is a documented marker of underdosing. At subtherapeutic levels, norepinephrine modulation, which drives energy and motivation, stays insufficient. Sertraline at 25 mg, for example, rarely produces the same energy-related improvements as the therapeutic range of 50 to 200 mg.
Sleep Problems Despite Antidepressant Use
Sleep problems despite antidepressant use beyond week 4 are a direct clinical signal. SSRIs at therapeutic doses typically normalize sleep architecture within 3 to 4 weeks. At low doses, REM sleep suppression is incomplete, and the brain’s sleep-wake cycle stays dysregulated. If sleep is still broken after a month on medication, dose is the first variable to examine.
Poor Concentration and Brain Fog
Cognitive symptoms like difficulty focusing, forgetfulness, and slow thinking are among the last to resolve, but they should show improvement by week 8. Persistent brain fog on antidepressants is a recognized marker of subtherapeutic dose antidepressant effects, particularly with medications that act on dopamine pathways, such as bupropion.
Anxiety Not Improving
SSRIs and SNRIs treat both depression and anxiety. If anxiety symptoms are unchanged or worsening after 6 weeks, that is a specific indicator of dose inadequacy. Anxiety pathways require consistent serotonin availability to downregulate. Inconsistent or low dosing fails to achieve that.
How to Tell If Your Dose Is Too Low vs Wrong Medication
Signs your antidepressant dose is too low versus the wrong medication show up in a specific pattern. If a patient had partial improvement in the first 2 to 4 weeks, which then plateaued, the dose is most likely too low. The drug is working; it just needs a higher concentration. If there was zero response after 8 weeks at a therapeutic dose, switching is appropriate.
Key differences at a glance:
- Partial improvement then plateau: Dose increase needed
- Zero response at full therapeutic dose after 8 weeks: Consider switching
- Side effects at low dose with no benefit: May indicate poor drug-gene compatibility (pharmacogenomic testing can identify this)
- Improvement that faded after months: Tolerance to antidepressants over time is the likely cause, not dose inadequacy from the start
- Anxiety worsened initially, then stabilized: Normal SSRI adjustment; not a dosing failure
- No improvement in sleep, energy, or mood after 6 weeks at starting dose: Classic symptoms of underdosed antidepressants
How Long Should Antidepressants Take to Work Properly
Most online sources say “4 to 6 weeks.” That is incomplete. The timeline has distinct stages, and knowing them prevents premature dose changes.
- Week 1 to 2: Sleep and appetite changes are the first to shift. Mood rarely changes yet. This is normal.
- Week 2 to 4: Energy and motivation begin improving. Anxiety often spikes briefly before improving. This is the phase where most patients wrongly assume the drug is not working.
- Week 4 to 6: Mood, concentration, and emotional regulation should show measurable improvement. If they do not, this is when signs your antidepressant dose is too low become clinically actionable.
- Week 6 to 8: Full therapeutic response. If symptoms remain at 60% to 70% of baseline severity, a dose increase is warranted before switching drugs.
The American Psychiatric Association guidelines state that dose optimization at the current medication should be attempted before switching to a new drug. Most patients are switched too quickly.
Sleep Problems Despite Antidepressant Use
Sleep problems despite antidepressant use are more common than most people realize, and more clinically significant than they are treated. A 2021 study in the Journal of Clinical Psychiatry found that 40% of patients on SSRIs reported ongoing sleep disturbance 8 weeks into treatment.
At subtherapeutic doses, two specific sleep problems persist:
- REM sleep disruption: SSRIs suppress REM at therapeutic doses. At low doses, this suppression is incomplete, causing fragmented, non-restorative sleep with vivid or disturbing dreams
- Sleep onset insomnia: Low serotonin availability at night delays the natural transition into sleep, even when the patient feels physically tired
Dose adjustment resolves the sleep disruption in most cases. Adding a sedative without addressing the underlying dose issue masks the symptom while the core problem continues.
Sleep problems despite antidepressant use that persist beyond 4 weeks are a direct reason to contact the prescribing doctor. Do not wait for the next scheduled appointment.
Tolerance to Antidepressants Over Time
Tolerance to antidepressants over time is a real and documented phenomenon, clinically known as tachyphylaxis or antidepressant poop-out. It affects an estimated 25% to 30% of long-term antidepressant users in the US.
It looks like this: the medication worked well for months or years, then symptoms gradually returned without any life change that would explain it. This is not relapse. The drug is no longer producing the same receptor response at the same dose.
Tolerance to antidepressants over time happens through two main mechanisms:
- Receptor downregulation: Long-term serotonin exposure causes the brain to reduce the number of active serotonin receptors, diminishing the drug’s effect
- CYP450 enzyme adaptation: The liver begins metabolizing the drug faster over time, reducing its effective blood concentration
The signs your antidepressant dose is too low due to tolerance are distinct from initial underdosing. Symptoms return gradually, not all at once. Energy typically drops first, then mood, then sleep. A dose increase or augmentation strategy (adding a second agent like bupropion or lithium) is the standard clinical response.
What Doctors Do When Your Dose Is Too Low
When signs your antidepressant dose is too low are confirmed, doctors follow a structured process. Self-adjusting doses is unsafe and a separate section below addresses why.
Gradual Dose Increase (Titration)
Doctors increase the dose in small steps, typically 25 mg to 50 mg increments for SSRIs, with 2 to 4 weeks between increases. This allows the body to adjust and minimizes side effects. Jumping to a maximum dose immediately raises the risk of serotonin syndrome and severe anxiety.
Monitoring Response and Side Effects
After each dose increase, the doctor tracks specific metrics: sleep quality, energy, mood on a standardized scale (PHQ-9 or HAM-D), and any new side effects. This is not just a check-in. It is a data-driven adjustment process.
Combination Therapy If Needed
If the maximum therapeutic dose of the current medication does not produce full response, doctors add an augmenting agent rather than switching. Aripiprazole, bupropion, and lithium are common additions that work alongside the primary antidepressant. Switching antidepressants if dose is low is the last step, not the first. Switching antidepressants if dose is low before maximizing the current drug is a documented clinical error that extends the period of illness.
Subtherapeutic dose antidepressant effects can be corrected without abandoning a medication that is partially working. Give the titration process its full timeline.
FAQs
What are the signs your antidepressant dose is too low?
The primary signs your antidepressant dose is too low are persistent low mood, fatigue, broken sleep, and unresolved anxiety beyond 6 to 8 weeks of use. Partial improvement that then plateaus is the clearest signal. Zero improvement after 8 weeks at a starting dose points to the same problem.
Can antidepressants work partially if the dose is too low?
Yes. At subtherapeutic doses, SSRIs partially inhibit serotonin reuptake but do not reach full receptor saturation. This produces 20% to 40% symptom improvement without full recovery. Partial response is the most common outcome of underdosing and the most frequent reason dose increases are needed.
How long should antidepressants take to fully work?
Full therapeutic response takes 6 to 8 weeks. Sleep and appetite improve first, around week 2. Energy improves by week 4. Mood and concentration reach maximum improvement by week 6 to 8. If these milestones are missed, signs your antidepressant dose is too low are present and need clinical review.
Why do I still have sleep problems despite antidepressants?
Sleep problems despite antidepressant use beyond week 4 indicate that serotonin availability at night is insufficient for REM regulation. This resolves with dose optimization in most cases. Adding a sleep medication without adjusting the antidepressant dose treats the symptom, not the cause.
What are symptoms of underdosed antidepressants?
Symptoms of underdosed antidepressants include emotional flatness, ongoing fatigue, poor focus, disrupted sleep, and anxiety that does not improve after 6 weeks. These differ from side effects because they represent the continued presence of the original condition, not a drug reaction.
Can you build tolerance to antidepressants over time?
Yes. Tolerance to antidepressants over time affects 25% to 30% of long-term users. It develops through receptor downregulation and faster liver metabolism of the drug. It presents as a gradual return of symptoms after months or years of stability, starting with energy loss before mood declines.
Should I increase my antidepressant dose on my own?
No. Self-adjusting antidepressant doses carries serious risks including serotonin syndrome, severe anxiety spikes, and cardiovascular effects. Dose changes require medical supervision, proper titration schedules, and monitoring. Contact the prescribing doctor when signs your antidepressant dose is too low are present.
When should you switch antidepressants if dose is low?
Switching antidepressants if dose is low is appropriate only after reaching the maximum therapeutic dose of the current medication with no meaningful response after 8 weeks. Switching before this point is a clinical error. Partial responders should have dose optimization attempted before any switch is considered.
What happens if you stay on a low antidepressant dose?
Subtherapeutic dose antidepressant effects that continue untreated increase the risk of chronic depression. A 2020 study in Lancet Psychiatry found that patients on low doses for over 6 months had 45% higher relapse rates than those on therapeutic doses. Prolonged underdosing also reduces the drug’s long-term effectiveness.
How do doctors adjust antidepressant doses safely?
Doctors use titration: small incremental increases (25 mg to 50 mg for SSRIs) every 2 to 4 weeks, with PHQ-9 tracking at each step. Maximum doses are reached only if lower doses fail. Augmentation with a second agent is considered before switching antidepressants if dose is low is recommended.











1 Comment
Comments are closed.