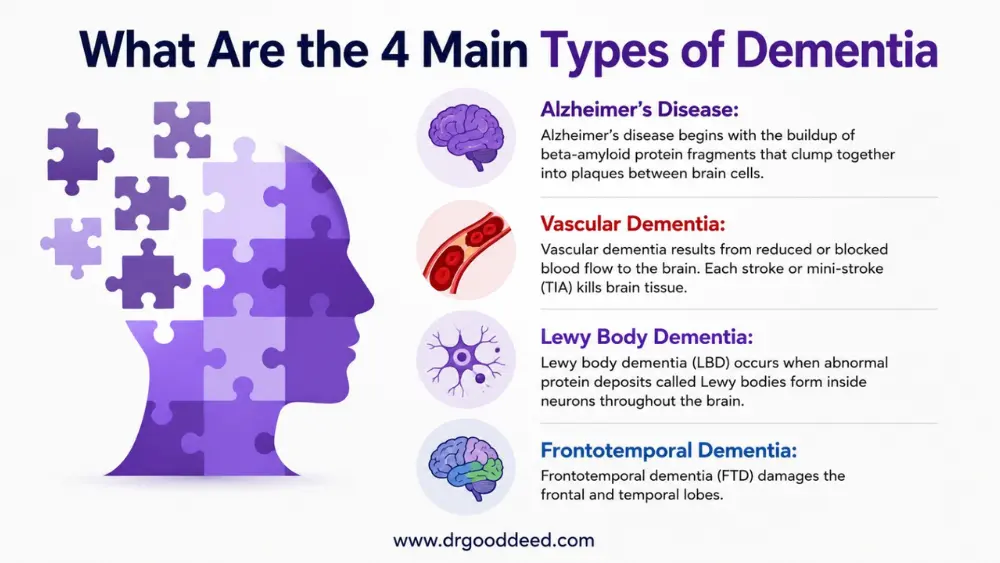
The 4 main types of dementia are Alzheimer’s disease, vascular dementia, Lewy body dementia, and frontotemporal dementia. Together, they account for the vast majority of dementia diagnoses in the USA, where over 6.9 million people currently live with Alzheimer’s alone, according to the Alzheimer’s Association 2024 report.
Dementia is not a single disease. It is a term for a group of symptoms caused by different types of brain damage.
This guide covers all four types of dementia in detail, including what happens in the brain, early warning signs, how each progresses, and what treatment options for major dementia types are currently available.
The 4 Main Types of Dementia at a Glance
| Type | Primary Brain Changes | Typical First Symptoms | Average Age of Onset |
| Alzheimer’s Disease | Amyloid plaques; tau tangles destroy neurons starting in the hippocampus | Memory loss for recent events; word-finding difficulty | 65+ (early-onset possible in 40s-50s) |
| Vascular Dementia | Strokes or reduced blood flow damage brain tissue | Slowed thinking; planning difficulty; walking problems | 60-75 |
| Lewy Body Dementia | Abnormal alpha-synuclein protein deposits in brain cells | Visual hallucinations; sleep disturbances; movement problems | 50-80 |
| Frontotemporal Dementia | Frontal and temporal lobe neuron loss | Personality shifts; language failure; impulsivity | 45-65 (youngest average onset) |
What Are the 4 Main Types of Dementia?
The 4 main types of dementia each have a distinct biological fingerprint. Knowing which type a person has is not just academic. It determines which medications help, which symptoms to anticipate, and how quickly families need to plan for increased care.
Alzheimer’s Disease
What Happens in the Brain?
Alzheimer’s disease begins with the buildup of beta-amyloid protein fragments that clump together into plaques between brain cells. Separately, a protein called tau misfolds and forms tangles inside neurons. Both plaques and tangles disrupt cell communication and eventually kill neurons. The hippocampus, the brain’s memory center, is the first region destroyed. Damage then spreads to the cortex, affecting language, reasoning, and personality.
Early Signs That Often Appear First
- Forgetting recent conversations or events while remembering older ones clearly
- Asking the same question multiple times within a short period
- Misplacing objects in unusual locations (putting keys in the refrigerator)
- Difficulty finding words mid-sentence
Distinguishing Feature
Memory failure is the dominant early symptom. Other cognitive functions stay relatively intact at first. The causes of Alzheimer’s disease involve a combination of genetics (especially the APOE-e4 gene variant), age, and lifestyle factors. A 2023 study in Nature Medicine confirmed that amyloid accumulation begins 15–20 years before symptoms appear, which is why early biomarker testing now matters.
Vascular Dementia
What Causes It?
Vascular dementia results from reduced or blocked blood flow to the brain. Each stroke or mini-stroke (TIA) kills brain tissue. The damage accumulates over time. Unlike Alzheimer’s, the injury is not from protein buildup but from oxygen deprivation. The areas damaged depend on where the strokes occur, which is why symptoms vary widely between patients.
Early Signs
- Slowed thinking and processing speed
- Difficulty with planning and organizing tasks
- Walking problems or a shuffling gait appearing early
- Urinary urgency or incontinence before significant memory loss
Distinguishing Feature
Decline happens in steps, not a steady slope. A person may stay stable for months, then drop sharply after a new stroke. Blood pressure control is the single most powerful treatment option for major dementia types in this category, reducing further stroke risk by up to 38%, per American Heart Association 2023 data.
Lewy Body Dementia
What Makes It Unique?
Lewy body dementia (LBD) occurs when abnormal protein deposits called Lewy bodies form inside neurons throughout the brain, including the cerebral cortex and brainstem. These deposits disrupt dopamine and acetylcholine signaling simultaneously. This dual disruption explains why LBD produces both cognitive symptoms (like dementia) and movement symptoms (like Parkinson’s disease) in the same person.
Early Signs
- Vivid, detailed visual hallucinations of people or animals, often appearing in the first year
- REM sleep behavior disorder: the person physically acts out dreams, sometimes violently
- Significant day-to-day fluctuation in alertness and attention
- Parkinson’s-like tremors or stiffness appearing alongside cognitive changes
Distinguishing Feature
Lewy body dementia signs are unique because memory may stay relatively preserved in early stages while hallucinations, sleep problems, and movement issues are already prominent. This is the reverse of Alzheimer’s. Critically, people with LBD have a severe and potentially fatal reaction to antipsychotic medications.
Haloperidol and similar drugs cause neuroleptic malignancy syndrome in LBD patients. This is a life-threatening emergency, and most LBD patients should never receive those drugs.
Frontotemporal Dementia
What Areas Are Affected?
Frontotemporal dementia (FTD) damages the frontal and temporal lobes. The frontal lobe controls personality, decision-making, impulse control, and social behavior. The temporal lobe handles language comprehension and word retrieval. Unlike the other 4 main types of dementia, FTD strikes a younger population, with most diagnoses occurring between ages 45 and 65.
Early Signs
- Sudden personality change: a previously reserved person becomes loud, inappropriate, or disinhibited
- Loss of empathy; no longer caring about others’ feelings
- Compulsive behaviors such as repeatedly doing the same thing
- Progressive loss of language in some subtypes (primary progressive aphasia)
Distinguishing Feature
Memory stays largely intact in early FTD. Families often notice behavioral or language changes months to years before any memory problem appears. Because of this, FTD is frequently misdiagnosed as a psychiatric condition, such as depression or bipolar disorder, before the correct diagnosis is made.
The Symptom Clues That Help Differentiate the Four Types of Dementia
Identifying which of the 4 main types of dementia a person has requires looking at the pattern of first symptoms carefully. These distinctions matter because misidentifying the type leads to wrong treatment decisions.
| Symptom | Most Likely Type |
| Memory loss as the very first symptom | Alzheimer’s disease |
| Personality change before memory loss | Frontotemporal dementia |
| Visual hallucinations within the first year | Lewy body dementia |
| Stepwise decline after strokes | Vascular dementia |
| Walking difficulty appearing early | Vascular or Lewy body dementia |
| Urinary incontinence before severe memory loss | Vascular dementia |
| Acting out dreams during sleep | Lewy body dementia |
| Language breakdown without memory loss | Frontotemporal dementia (language subtype) |
How Progression Differs Among the Four Types
Progression speed and pattern differ significantly across the 4 main types of dementia.
Alzheimer’s disease progresses slowly and continuously. From mild symptoms to end-stage typically spans 8–10 years, though some cases extend to 20 years. Decline is gradual with no stable plateaus.
Vascular dementia progresses in steps. Each new stroke or TIA causes a sudden drop in function. Between strokes, the person may stay stable for six to eighteen months. Overall survival from diagnosis averages 5–7 years, though this varies heavily with cardiovascular risk control.
Lewy body dementia progresses faster than Alzheimer’s on average. Most patients reach severe impairment within 5–7 years of diagnosis. Fluctuations in alertness can be dramatic day to day, making care planning more complex.
Frontotemporal dementia has the widest variation. Some behavioral subtypes progress over 6–8 years. Primary progressive aphasia subtypes may progress faster, losing language almost entirely within 3–4 years while mobility stays intact longer.
How One Patient’s Lewy Body Dementia Was Mismanaged Before the Correct Diagnosis Changed Everything
Privacy Note: The following case is a realistic composite based on documented clinical presentations of Lewy body dementia. The patient’s name has been altered to protect privacy.
Franklin Osei, a 74-year-old retired engineer from Atlanta, Georgia, began experiencing vivid hallucinations in early 2021. He described seeing small children in his living room who were not there. His family also noticed he had started acting out his dreams at night, sometimes shouting and swinging his arms in bed. His primary care physician referred him to a psychiatrist, who diagnosed late-onset psychosis and prescribed haloperidol.
Within 48 hours of starting haloperidol, Franklin became rigidly stiff, developed a high fever, and stopped responding to questions. His family brought him to the emergency room at Emory University Hospital. The attending neurologist recognized the presentation immediately as neuroleptic malignancy syndrome triggered by antipsychotic use in a patient with Lewy body dementia signs.
The haloperidol was stopped. Franklin received supportive care and stabilized over several days. A full neurological evaluation confirmed Lewy body dementia based on his hallucinations, REM sleep behavior disorder history, fluctuating alertness, and mild parkinsonian tremor on examination. His DaTscan imaging showed reduced dopamine transporter activity consistent with LBD.
The detail most articles miss: his treatment team switched him to quetiapine at a very low dose (12.5 mg), which is one of the few antipsychotics considered relatively safer in LBD when hallucinations are severely distressing. They also started rivastigmine (a cholinesterase inhibitor), which has FDA approval for Parkinson’s disease dementia and clinical evidence supporting its use in LBD. His hallucinations reduced in frequency within six weeks without triggering further motor complications.
Franklin’s family enrolled in the Lewy Body Dementia Association caregiver program and learned to structure his daily schedule to match his better alertness windows in the morning. His case is a textbook example of why type-specific diagnosis in the 4 main types of dementia is not optional.
Can Someone Have More Than One Type of Dementia?
Yes. Mixed dementia, meaning the presence of two or more types of dementia simultaneously, is more common than most people realize. Autopsy studies show that nearly half of all dementia patients over age 80 have brain changes from more than one dementia type, most commonly Alzheimer’s combined with vascular dementia. A 2020 study in Brain found that 45% of donated brains from dementia patients showed pathology consistent with multiple dementia types.
Mixed dementia is harder to diagnose during life because the symptoms overlap. It also tends to progress faster than single-type dementia. Managing symptoms of dementia in mixed cases requires addressing risk factors from both types simultaneously, such as controlling blood pressure while also using cholinesterase inhibitors for the Alzheimer’s component.
Risk Factors for Dementia
Risk factors vary somewhat by type but share a significant overlap across all 4 main types of dementia.
Non-modifiable risk factors:
- Age over 65 (risk doubles every five years after 65)
- APOE-e4 gene variant (increases Alzheimer’s risk 3–5 times in one copy; 8–12 times in two copies)
- Family history of dementia
- Down syndrome (nearly all develop Alzheimer’s pathology by age 40)
Modifiable risk factors (The Lancet Commission 2024 identified 14 factors accounting for 45% of dementia cases):
- Uncontrolled hypertension in midlife
- Type 2 diabetes
- Obesity
- Physical inactivity
- Excessive alcohol consumption (more than 14 units per week)
- Smoking
- Depression
- Social isolation
- Hearing loss (untreated hearing loss increases dementia risk by 90%, per The Lancet 2020)
- Low education level in early life
- Traumatic brain injury
- Air pollution exposure
- Untreated vision loss
- High LDL cholesterol (newly added in 2024 update)
Treatment options for major dementia types currently do not include a cure, but managing these modifiable risk factors reduces the overall population burden of dementia significantly.
FAQs
What causes Alzheimer’s disease?
The causes of Alzheimer’s disease include beta-amyloid plaques, tau tangles, and the APOE-e4 gene variant. Amyloid accumulation begins 15–20 years before symptoms. Age is the strongest risk factor. Lifestyle factors, including hypertension, inactivity, and social isolation each independently raise risk.
How is vascular dementia different from Alzheimer’s disease?
Vascular dementia results from stroke-related brain damage; Alzheimer’s results from amyloid plaques and tau tangles. Among the 4 main types of dementia, vascular dementia is the only type where aggressive blood pressure control can meaningfully slow progression. Memory loss is less prominent early in vascular dementia.
Can a person have more than one type of dementia?
Yes. Mixed dementia affects nearly 45% of dementia patients over 80, per autopsy data from Brain (2020). Alzheimer’s combined with vascular dementia is the most common mixed presentation. It progresses faster and is harder to diagnose during life than single-type dementia.
How are the major types of dementia diagnosed?
Diagnosis involves neuropsychological testing, brain MRI or CT scan, blood tests to rule out reversible causes, and sometimes PET imaging or cerebrospinal fluid biomarkers. DaTscan imaging is specific to confirming Lewy body dementia signs. No single test diagnoses all 4 main types of dementia.
Can dementia be cured?
No. None of the 4 main types of dementia are currently curable. Lecanemab (Leqembi) and donanemab slow Alzheimer’s progression modestly in early stages. Vascular dementia progression can be slowed by stroke prevention. All other treatment options for major dementia types manage symptoms only.
How can families help manage symptoms of dementia?
Managing symptoms of dementia at home involves structured daily routines, safety-proofing the living environment, using visual cues and labels, maintaining physical activity, and reducing sensory overstimulation. Caregiver education programs through the Alzheimer’s Association reduce patient behavioral symptoms by up to 40% in some studies.
What lifestyle changes may support brain health?
150 minutes of moderate aerobic exercise weekly, a Mediterranean-DASH diet, treating hearing loss with hearing aids, maintaining social connections, and controlling blood pressure below 130/80 mmHg all reduce dementia risk. These apply across all types of dementia with a vascular or lifestyle component.
When should someone seek medical evaluation for memory loss?
Seek evaluation immediately if memory lapses affect daily function, if personality changes appear suddenly, if a person gets lost in familiar places, or if visual hallucinations are present. Early diagnosis of the 4 main types of dementia allows earlier access to medications and care planning.
How quickly do different types of dementia progress?
Alzheimer’s: 8–10 years average from diagnosis to end-stage. Vascular dementia: 5–7 years with stepwise decline. Lewy body dementia: 5–7 years with rapid fluctuations. Frontotemporal dementia: 6–8 years for behavioral subtypes; 3–4 years for some language subtypes.
References
- Alzheimer’s Association. 2024 Alzheimer’s Disease Facts and Figures.
- Hampel H, et al. Amyloid accumulation timeline in Alzheimer’s disease. Nature Medicine. 2023.
- American Heart Association. Vascular Dementia and Blood Pressure Guidelines. 2023.
- Lewy Body Dementia Association. Antipsychotic Sensitivity in LBD. 2023.
- Kapasi A, et al. Mixed dementia pathology prevalence in aging brains. Brain. 2020.
- Livingston G, et al. Dementia prevention, intervention, and care: 2024 Lancet Commission report. The Lancet. 2024.
- National Institute on Aging. What Is Frontotemporal Dementia? 2023.
- McKeith IG, et al. Diagnosis and management of dementia with Lewy bodies. Neurology. 2020.