Understanding what separates Alzheimer’s from other forms of dementia can change how you look out for symptoms, push for early diagnosis, and make informed care decisions. In 2025, an estimated 7.2 million Americans aged 65 and older are living with Alzheimer’s dementia, according to the Alzheimer’s Association.
This guide covers everything you need to know about alzheimer’s vs dementia, including symptoms, causes, risk factors, diagnostic tools, and treatment options.
Difference Between Alzheimer’s and Dementia
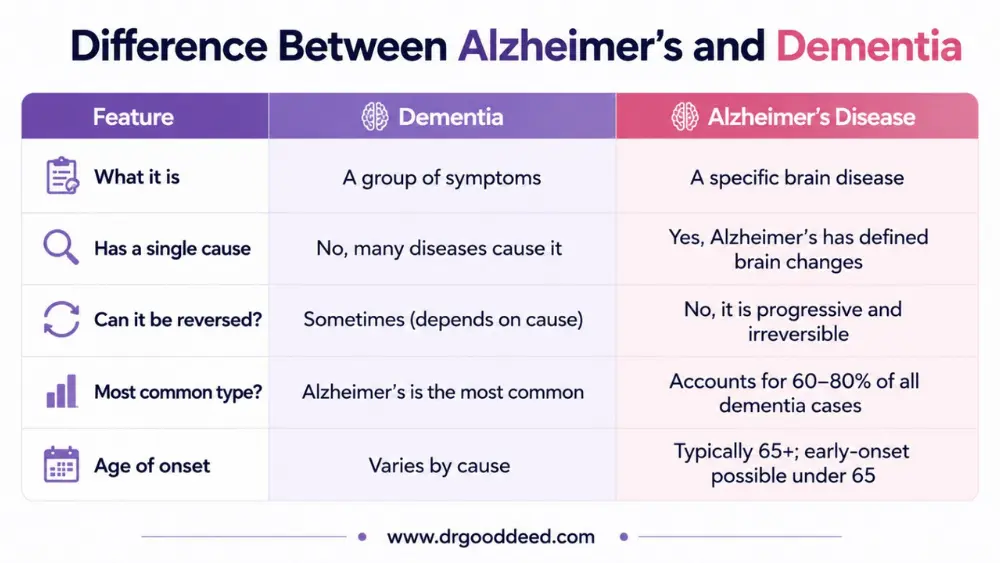
Dementia is a group of symptoms, and Alzheimer’s is a specific brain disease. Dementia is not a diagnosis on its own. It is an umbrella term for a decline in memory, thinking, and reasoning severe enough to affect daily life.
Alzheimer’s disease is one cause of dementia, and the most common one. Put plainly, every case of Alzheimer’s produces dementia, but not every dementia comes from Alzheimer’s.
| Feature | Dementia | Alzheimer’s Disease |
| What it is | A group of symptoms | A specific brain disease |
| Has a single cause | No, many diseases cause it | Yes, Alzheimer’s has defined brain changes |
| Can it be reversed? | Sometimes (depends on cause) | No, it is progressive and irreversible |
| Most common type? | Alzheimer’s is the most common | Accounts for 60–80% of all dementia cases |
| Age of onset | Varies by cause | Typically 65+; early-onset possible under 65 |
Dementia Is a Syndrome, Not a Single Disease
A syndrome is a collection of symptoms that occur together. Dementia is defined by at least two of the following: memory loss, trouble with language, difficulty reasoning, changes in personality, or problems with coordination. These symptoms must be severe enough to interfere with daily life. Dementia can result from Alzheimer’s disease, strokes, Lewy body protein deposits, or even vitamin B12 deficiency.
Some dementia causes are reversible. A thyroid disorder or medication side effect can mimic dementia. That is why a full medical evaluation always matters before any diagnosis.
Alzheimer’s Is One Specific Disease That Causes Dementia
Alzheimer’s disease causes physical changes in the brain, specifically the buildup of amyloid plaques between neurons and tau tangles inside neurons. These changes disrupt how brain cells communicate, and eventually cause them to die. The damage spreads progressively. There is currently no way to reverse this process, though two FDA-approved drugs now slow it in its early stages.
Alzheimer’s Symptoms vs Dementia Symptoms
Many symptoms overlap, but there are tell-tale signs that point more specifically toward Alzheimer’s. Not all memory loss is Alzheimer’s, and not all Alzheimer’s looks the same.
Early Memory Loss
In Alzheimer’s, recent memory fails first. A person forgets a conversation that happened an hour ago but can clearly recall a wedding from 40 years back. This is because Alzheimer’s first damages the hippocampus, the brain’s memory-forming center. Vascular dementia, by contrast, typically impairs planning and processing speed before memory.
Difficulty Learning New Information
Alzheimer’s makes it hard to absorb and retain new information. A person might ask the same question several times in a single afternoon, not realizing they already asked it. This is distinct from normal aging, where forgetfulness is occasional and the person often recalls things with a prompt.
Language and Communication Problems
Word-finding difficulty is common in Alzheimer’s. A person may stop mid-sentence, searching for a word they have used all their life. In frontotemporal dementia (FTD), by contrast, language breaks down differently. Some people with FTD lose the ability to understand word meanings rather than retrieve them.
Confusion and Disorientation
People with Alzheimer’s often get lost in familiar places, like their own neighborhood. They may not recognize what day, month, or year it is. In Lewy body dementia, confusion comes in waves. A person can seem perfectly clear in the morning and deeply confused by afternoon.
Behavioral and Personality Changes
In Alzheimer’s, personality changes tend to emerge in the middle stages. A previously calm person may become anxious, suspicious, or easily upset. Frontotemporal dementia is different: personality and behavior changes often show up first, before any memory problems appear.
Difficulty Performing Daily Activities
As alzheimer’s vs dementia progresses in either form, managing daily tasks becomes harder. Driving, managing finances, cooking, and keeping appointments all become difficult. In Alzheimer’s, this usually follows memory decline. In some other dementias, it can be the very first symptom.
Causes of Alzheimer’s Disease
The causes of Alzheimer’s disease involve specific biological changes in the brain that researchers now understand far better than they did a decade ago.
Amyloid Plaques and Tau Tangles
The two hallmark changes are amyloid plaques and tau tangles. Amyloid beta protein clumps together between neurons, blocking communication signals. Inside the neurons, tau protein collapses into twisted tangles, cutting off the cell’s internal transport system. Both changes starve neurons of nutrients and eventually kill them.
Brain Cell Damage
Alzheimer’s kills neurons in a pattern. It starts in the hippocampus and entorhinal cortex, both critical for memory formation. Over time, it spreads to the cortex, affecting reasoning, language, and judgment. By the late stage, the brain may lose significant volume, visible on an MRI scan.
Genetic Influences
The APOE e4 gene is the strongest known genetic risk factor. Inheriting one copy from a parent raises risk; two copies raises it further. A rare form of Alzheimer’s, early-onset familial Alzheimer’s, is directly caused by mutations in the PSEN1, PSEN2, or APP genes. This accounts for less than 1% of all Alzheimer’s cases.
Age-Related Brain Changes
The biggest risk factor is age. The risk of Alzheimer’s roughly doubles every five years after age 65. By age 85, about one in three people has Alzheimer’s. The aging brain clears amyloid less efficiently, allowing plaques to accumulate over many years before symptoms appear.
Ongoing Research Into Causes
Researchers are now studying neuroinflammation as a key driver of Alzheimer’s damage, not just a side effect. Microglia, the brain’s immune cells, may misfire and attack healthy tissue alongside amyloid. Studies published in Nature Neuroscience and The Lancet Neurology between 2022 and 2024 have supported this as a secondary disease pathway worth targeting with future drugs.
Risk Factors for Dementia and Alzheimer’s
The risk factors for dementia and Alzheimer’s include factors you cannot change and some that you can actively modify. Knowing where you stand is the first step in reducing risk. The difference between Alzheimer’s and dementia risk profiles matters here too: some risks are universal, others are type-specific.
Fixed risk factors:
- Age (most significant factor; risk increases sharply after 65)
- Family history and genetic variants like APOE e4
- Down syndrome (almost all people with Down syndrome develop Alzheimer’s pathology by age 40)
- History of traumatic brain injury
Modifiable risk factors (evidence-supported):
- Uncontrolled high blood pressure in midlife
- Type 2 diabetes
- Obesity
- Physical inactivity
- Chronic sleep deprivation (disrupts amyloid clearance during sleep)
- Hearing loss left untreated
- Social isolation and depression
- Heavy alcohol use and smoking
A 2020 Lancet Commission report identified 12 modifiable risk factors for dementia and Alzheimer’s that together account for approximately 40% of dementia cases worldwide. Addressing these in midlife has real preventive potential. This is one area where the alzheimer’s vs dementia conversation becomes very practical.
How Doctors Tell Alzheimer’s Apart from Other Dementias
Diagnosing alzheimer’s vs dementia type requires more than a memory test. No single test confirms Alzheimer’s during life. Here is how doctors work through it:
- Cognitive tests such as the Mini-Mental State Examination (MMSE) or the Montreal Cognitive Assessment (MoCA) to measure reasoning and memory
- Blood tests to rule out reversible causes (thyroid disease, vitamin deficiencies, infections)
- MRI or CT scans to detect brain shrinkage, strokes, or tumors
- PET scans to detect amyloid buildup in the brain (now partially replaceable by blood tests approved in 2024 that match PET accuracy over 90% of the time)
- Cerebrospinal fluid tests for amyloid and tau protein levels
Lewy body dementia often causes early visual hallucinations and Parkinson-like tremors. Frontotemporal dementia causes personality shifts before memory loss. Vascular dementia often follows a stroke and progresses in steps rather than gradually.
Treatment Differences Between Dementia and Alzheimer’s
When it comes to alzheimer’s vs dementia, treatment is where the distinction becomes most critical. The treatment options for Alzheimer’s disease now include therapies that go beyond symptom management for the first time in decades.
Treatments That Target Alzheimer’s Disease
Two drugs have received full FDA approval as disease-modifying therapies:
- Lecanemab (Leqembi), approved July 2023, clears amyloid plaques and slowed cognitive decline by about 27% in clinical trials. It is given as an IV infusion every two weeks. As of January 2025, a once-monthly maintenance dosing option is also approved.
- Donanemab (Kisunla), approved July 2024, is given monthly and showed up to 35% slowing of decline in early-stage patients in the TRAILBLAZER-ALZ 2 trial. Treatment may be paused once scans show amyloid is cleared.
Both drugs are limited to early-stage patients with confirmed amyloid buildup. Neither works on moderate or advanced Alzheimer’s.
Older symptom-management drugs are still used alongside these:
- Cholinesterase inhibitors (donepezil, rivastigmine, galantamine) improve communication between neurons
- Memantine helps regulate glutamate activity to reduce confusion
Dementia Treatment Depends on the Cause
The treatment options for Alzheimer’s disease do not apply to all dementia types. A person with vascular dementia needs blood pressure control and stroke prevention. Someone with Lewy body dementia benefits from specific Parkinson’s medications but must avoid certain antipsychotics, which can cause a life-threatening reaction. Dementia caused by a B12 deficiency or thyroid disease can be reversed by treating the underlying condition. No one treatment plan covers all dementia types.
When Memory Loss Is Not Dementia
Understanding alzheimer’s vs dementia also means knowing what neither of them looks like. Not every memory problem means dementia or Alzheimer’s. The following can cause memory and thinking problems that fully resolve:
- Depression: Severe depression impairs concentration and memory in a way that closely mimics early dementia
- Sleep deprivation: Chronic poor sleep reduces processing speed and recall significantly
- Medication side effects: Sedatives, antihistamines, and some blood pressure drugs affect cognition
- Thyroid dysfunction: Both overactive and underactive thyroid glands impair thinking
- Vitamin B12 deficiency: A common cause of reversible cognitive decline in older adults
If symptoms come on suddenly or fluctuate dramatically, that points more toward a reversible cause. Gradual, consistent worsening over months to years is a red flag for progressive dementia.
FAQs
Is Alzheimer’s disease a type of dementia?
Yes. Alzheimer’s disease is the most common type of dementia, responsible for 60–80% of all cases in the US. It causes specific brain changes (amyloid plaques and tau tangles) that other dementias do not.
Which comes first, Alzheimer’s or dementia?
Neither comes “first” in the way the question implies. Alzheimer’s disease is the cause; dementia is the symptom set that results. Brain changes from Alzheimer’s start 10–20 years before any symptoms appear.
Can someone have dementia without Alzheimer’s disease?
Yes. Vascular dementia, Lewy body dementia, and frontotemporal dementia are all distinct causes of dementia with no Alzheimer’s pathology required. Some people have mixed dementia with two types simultaneously.
What are the major risk factors for dementia and Alzheimer’s?
Age is the strongest risk factor. After 65, risk doubles every five years. Carrying the APOE e4 gene, untreated high blood pressure, Type 2 diabetes, social isolation, and chronic sleep deprivation are all evidence-supported modifiable risk factors for dementia and Alzheimer’s.
Is memory loss always a sign of Alzheimer’s disease?
No. Depression, B12 deficiency, thyroid disorders, medication side effects, and sleep deprivation all cause fully reversible memory problems. When comparing Alzheimer’s symptoms vs dementia symptoms, Alzheimer’s memory loss is progressive, starts with recent events, and does not improve without disease-modifying treatment.
How quickly does Alzheimer’s disease progress?
The average time from diagnosis to late-stage Alzheimer’s is 8–10 years, but the range is 3–20 years. People diagnosed under 65 (early-onset) often experience faster progression. Understanding the causes of Alzheimer’s disease, like genetic risk and amyloid burden, can help predict trajectory.
Can lifestyle changes reduce dementia risk?
Yes. The 2020 Lancet Commission found 12 modifiable risk factors account for 40% of dementia cases. Regular aerobic exercise, hearing aid use for untreated hearing loss, managing blood pressure before age 60, and maintaining social connections all show evidence-supported risk reduction.
Sources
- Alzheimer’s Association. 2025 Alzheimer’s Disease Facts and Figures. Alzheimer’s & Dementia, 2025.
- National Institute on Aging. Understanding Different Types of Dementia. NIH.
- Livingston G, et al. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. The Lancet, 2020.
- Van Dyck CH, et al. Lecanemab in early Alzheimer’s disease. New England Journal of Medicine, 2023.
- Sims JR, et al. Donanemab in early symptomatic Alzheimer disease: The TRAILBLAZER-ALZ 2 randomized clinical trial. JAMA, 2023.
- FDA approval of lecanemab (Leqembi). U.S. Food and Drug Administration, 2023.
- FDA approval of donanemab (Kisunla). U.S. Food and Drug Administration, July 2, 2024.
- Alzheimer’s Association. Lecanemab (Leqembi) Approved for Alzheimer’s. alz.org.
- Lewy Body Dementia Association. Is It LBD or Something Else?