Yes, it is clinically confirmed that allergies can cause headaches. Allergic rhinitis triggers inflammation in the nasal passages and sinuses, blocking drainage and building pressure that produces head pain.
The American College of Allergy, Asthma, and Immunology (ACAAI) estimates that over 50 million people in the USA experience allergies annually, and sinus-related headache is among the most common complaints during allergy season.
Can Seasonal Allergies Trigger Headaches?
Seasonal allergies can trigger headaches. Pollen lands on the nasal mucosa, triggers IgE-mediated mast cell degranulation, and floods the nasal tissue with histamine. Histamine causes vasodilation and mucosal swelling.
Swollen tissue blocks sinus drainage channels. Trapped mucus and air pressure changes inside the sinuses produce pain. This process takes less than 20 minutes after allergen exposure in sensitized individuals.
Pollen and Seasonal Allergy Triggers
Tree pollen (birch, oak, cedar) peaks in March through May. Grass pollen peaks June through August. Ragweed dominates August through October. Each triggers the same histamine-mediated sinus response.
Pollen counts above 500 grains per cubic meter, a threshold used by the National Allergy Bureau, correlate with increased headache frequency in allergic rhinitis patients.
Spring and Fall Allergy Seasons
Spring allergies from tree and grass pollen produce frontal sinus headaches and orbital pressure. Fall allergies from ragweed produce more diffuse facial pain because ragweed pollen particles are smaller and penetrate deeper into nasal passages.
In the USA, ragweed season now runs 27 days longer than it did in 1995 due to climate-driven pollen season extension, per the Asthma and Allergy Foundation of America (AAFA).
Weather Changes and Headache Risk
Barometric pressure drops that accompany weather fronts reduce atmospheric pressure against sinuses, allowing swollen mucosa to expand further and intensifying sinus headache pain.
Patients with allergic rhinitis are significantly more sensitive to barometric pressure changes than non-allergic individuals, per research published in the International Journal of Biometeorology (Kimoto et al., 2011).
Seasonal Allergies and Migraine Flare-Ups
A 2016 study by Martin et al. published in Cephalalgia found that allergic rhinitis patients had migraine 5.6 times more often than controls without allergies. The mechanism is neurogenic: histamine directly activates trigeminal nerve fibers, which is the same neural pathway involved in migraine attacks. Allergy season correlates with measurable migraine frequency increases in susceptible individuals.
Nasal Congestion and Pressure Headaches
Nasal congestion and pressure headaches develop when swollen nasal tissue blocks the ostia, the small drainage openings connecting sinuses to the nasal cavity. Each sinus requires free drainage to equalize pressure.
When drainage stops, negative pressure builds inside the sinus cavity, creating suction-like pain against the sinus walls. Mucosal edema from allergies blocks ostia faster than infection, because allergic swelling is diffuse rather than localized.
How Congestion Affects Sinus Drainage
The ostiomeatal complex is the primary drainage hub for the maxillary, frontal, and anterior ethmoid sinuses. When allergic inflammation swells the middle turbinate and nasal mucosa, this drainage corridor narrows. Secretions accumulate.
The trapped mucus creates a growth environment for secondary bacterial infections, which intensifies pressure headaches and transforms an allergy headache into a full sinus infection headache.
Pressure Changes Within the Sinuses
Inside healthy sinuses, pressure stays close to atmospheric baseline. Blocked sinuses create a negative pressure differential of 10–30 mmHg below atmospheric pressure, per pressure measurements in patients with chronic rhinosinusitis. This pressure differential causes the tissue lining the sinus to be pulled inward, which is what produces the deep, throbbing quality of sinus headaches.
Common Areas of Pain
Forehead
Frontal sinus pain sits above the eyebrows and worsens when bending forward. The frontal sinuses drain via a long, narrow duct that clogs quickly with even mild mucosal swelling.
Around the Eyes
Ethmoid sinus pain produces pain between and behind the eyes. The ethmoid sinuses are the most numerous and smallest sinuses, making them prone to pressure buildup from minimal swelling.
Cheeks and Nose
Maxillary sinus pain produces cheek tenderness, upper tooth pain, and pain radiating across the nose bridge. The maxillary sinuses are the largest facial sinuses, holding the most volume of pressurized air and mucus.
Headache Symptoms From Allergies
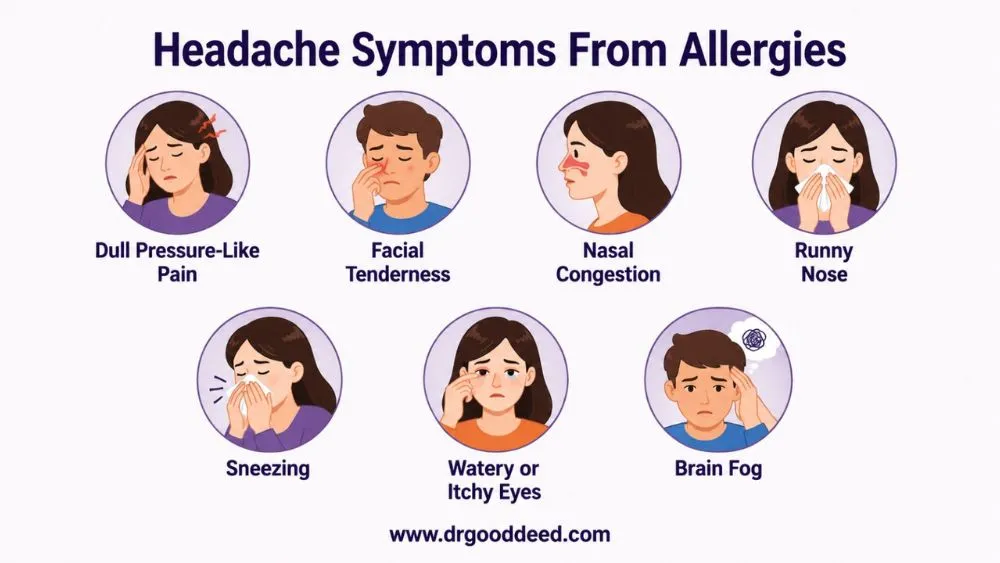
Headache symptoms from allergies differ from tension headaches and standard migraines in consistent ways.
Dull Pressure-Like Pain
Allergy headaches produce a constant, dull pressure rather than a pulsating pain. The pain stays steady regardless of activity level. This distinguishes it from migraine, which typically worsens with physical activity.
Facial Tenderness
Tapping the forehead, cheeks, or sinus areas with fingertips causes localized tenderness in allergy headaches. This tenderness reflects inflamed sinus walls. Tension headaches produce scalp muscle tenderness, not facial bone tenderness.
Nasal Congestion
Active nasal congestion accompanies allergy headaches in nearly all cases. Isolated head pain without concurrent nasal symptoms is rarely an allergy headache; other causes should be considered.
Runny Nose
Anterior rhinorrhea (clear, thin nasal discharge) accompanies allergic inflammation. Thick, colored discharge suggests bacterial superinfection has developed on top of the allergic base.
Sneezing
Repeated sneezing temporarily increases intracranial pressure by 20–40 mmHg per sneeze event, briefly intensifying headache pain. Patients often notice headache worsening during sneezing episodes.
Watery or Itchy Eyes
Allergic conjunctivitis co-occurs with allergic rhinitis in about 70% of patients. Itchy, watery eyes alongside a sinus headache strongly indicate an allergic rather than infectious cause.
Fatigue and Brain Fog
Histamine release during allergic reactions crosses the blood-brain barrier and reduces alertness. A 2018 meta-analysis in Clinical and Experimental Allergy confirmed that allergic rhinitis patients show measurably impaired cognitive performance, equivalent to mild alcohol intoxication, during active allergy symptoms.
Common Allergy Triggers Linked to Headaches
Allergy triggers linked to sinus inflammation causing headaches in the USA vary by season, geography, and indoor exposure. Identifying specific triggers through allergy testing is the only reliable path to targeted treatment.
Common triggers with documented sinus headache links:
- Ragweed pollen: The most prevalent outdoor allergen in the USA. Affects 23 million Americans. September peak correlates with highest allergy-headache emergency visits annually.
- Dust mites: The leading indoor allergen. Live in bedding, carpets, and upholstered furniture. Trigger perennial allergic rhinitis and year-round nasal congestion and pressure headaches.
- Pet dander: Cat allergen (Fel d 1) is aerodynamically light and stays airborne for hours. Dog dander (Can f 1) settles faster but persists on surfaces for months.
- Mold spores: Peak outdoors in late summer and fall. Produce perennial indoor symptoms from bathroom, basement, and HVAC mold.
- Cockroach allergen: Prevalent in urban USA housing, especially in the South. A major but underappreciated trigger for sinus inflammation causing headaches in inner-city populations.
- Tree pollen (birch, oak, cedar): Spring triggers that produce cross-reactivity with certain foods through oral allergy syndrome.
Risk Factors for Allergy-Related Headaches
Not every allergy patient develops significant headaches. These risk factors increase the likelihood:
- Personal or family history of allergic rhinitis, asthma, or eczema (atopic triad)
- Pre-existing migraine disorder, which shares trigeminal sensitization with allergy
- Deviated nasal septum or nasal polyps, which narrow baseline sinus drainage
- Chronic sinusitis, defined as sinus inflammation lasting 12 weeks or more
- Living in high-pollen geographic regions (Southeast and Midwest USA)
- Aspirin-exacerbated respiratory disease (AERD), which amplifies sinus inflammation
- Frequent use of over-the-counter nasal decongestant sprays, causing rebound congestion (rhinitis medicamentosa) after 3 days of use
How Allergies Are Diagnosed
Diagnosing allergies that cause headaches in a specific patient requires identifying both the allergic sensitization pattern and confirming that headaches correlate with allergen exposure rather than independent causes.
Diagnostic steps used by allergists and otolaryngologists:
- Skin prick testing: Gold standard. 50+ allergens applied simultaneously. Results in 15–20 minutes. Sensitivity above 85% for airborne allergens per ACAAI guidelines.
- Specific IgE blood testing (ImmunoCAP): Used when skin testing is not possible. Measures allergen-specific antibody levels. Slightly less sensitive than skin testing but highly specific.
- Nasal endoscopy: Allows direct visualization of nasal polyps, mucosal swelling, and drainage blockage. Performed in-office by ENT specialists.
- CT sinus imaging: Identifies sinus anatomy abnormalities and chronic mucosal thickening. Recommended when symptoms do not respond to standard allergy treatment within 4–6 weeks.
- Symptom diary: Patients record headache onset relative to outdoor activities, weather, and home exposures. This correlation data is diagnostic for headache symptoms from allergies when testing results are ambiguous.
- Headache diary cross-reference: Comparing headache frequency data with local pollen count data from the National Allergy Bureau database confirms seasonal allergy as the headache driver.
How to Relieve Allergy Headaches
Relieving allergy effectively requires for home care addressing both allergic inflammation and sinus pressure simultaneously.
Reducing Allergen Exposure
Stay indoors between 5–10 AM when pollen counts peak. Use HEPA filters in HVAC systems rated MERV 13 or higher. Keep windows closed during high-pollen days. Shower after outdoor activities to remove pollen from skin and hair before it transfers to bedding.
Antihistamine Medications
Second-generation antihistamines (cetirizine, fexofenadine, loratadine) block H1 receptors without crossing the blood-brain barrier at standard doses, making them non-sedating. They reduce nasal itching, sneezing, and watery eyes within 1–3 hours. They do not reliably reduce nasal congestion, which is the primary driver of sinus pressure headaches.
Nasal Corticosteroid Sprays
Fluticasone propionate, mometasone furoate, and budesonide are OTC nasal sprays that reduce sinus mucosal inflammation. They are the single most effective treatment for allergic rhinitis per ACAAI and AAAAI joint guidelines. Full effect takes 2–4 weeks of daily use. They directly address the mucosal swelling causing sinus drainage blockage.
Saline Nasal Irrigation
Neti pot or squeeze bottle saline irrigation physically flushes allergens and mucus from nasal passages. A 2007 Cochrane review confirmed saline irrigation reduces nasal symptom scores and improves sinus drainage. Use distilled or boiled and cooled water only; tap water carries infection risk. Irrigate once or twice daily during active allergy season.
Staying Hydrated
Adequate hydration (eight 8-ounce glasses of water daily) keeps nasal mucus thin and drainable. Thick mucus from dehydration worsens sinus blockage and intensifies pressure headaches. Caffeine and alcohol both promote dehydration and should be limited during active allergy flares.
Rest and Symptom Management
Sleeping with the head elevated 30–45 degrees improves sinus drainage by gravity. Warm compresses applied to the forehead and cheeks for 10–15 minutes reduce sinus wall tension and provide temporary headache relief.
Treatment Options for Allergy-Related Headaches
Over-the-Counter Allergy Medications
Oral decongestants (pseudoephedrine) reduce nasal mucosal swelling faster than antihistamines for headache relief. Pseudoephedrine is kept behind pharmacy counters in the USA per the Combat Methamphetamine Epidemic Act. It is not recommended for patients with high blood pressure, heart disease, or hyperthyroidism.
Prescription Allergy Treatments
Montelukast (Singulair) blocks leukotriene receptors, reducing both nasal and lower airway inflammation. Ipratropium bromide nasal spray reduces rhinorrhea effectively when antihistamines fail. Combination intranasal fluticasone-azelastine (Dymista) outperforms either agent alone in reducing total nasal symptom scores in clinical trials.
Immunotherapy (Allergy Shots)
Subcutaneous immunotherapy (SCIT) is the only treatment that modifies the underlying allergic disease rather than managing symptoms. The AAAAI confirms 85% of allergic rhinitis patients show significant improvement after completing 3–5 years of immunotherapy.
Sublingual immunotherapy tablets (SLIT) are FDA-approved for grass and ragweed allergies and are taken at home. Immunotherapy reduces sinus inflammation causing headaches by progressively reducing IgE-mediated mast cell reactivity.
Migraine Treatment When Needed
When allergy-associated headaches fulfill International Headache Society (IHS) criteria for migraine, triptan medications (sumatriptan, rizatriptan) are appropriate. Triptans do not treat the underlying allergic mechanism, so allergy management must continue in parallel. NSAIDs (ibuprofen, naproxen) reduce both sinus inflammation and headache pain simultaneously and are the first-line analgesic for allergy headaches.
Managing Chronic Sinus Inflammation
Chronic rhinosinusitis with nasal polyps responds to dupilumab (Dupixent), an IL-4/IL-13 receptor antagonist. The FDA approved dupilumab for chronic rhinosinusitis with nasal polyps in 2019. Clinical trials showed a 51% reduction in nasal polyp score and significant improvement in sinus congestion within 24 weeks. Functional endoscopic sinus surgery (FESS) widens sinus drainage channels when medical therapy fails.
Preventing Allergy Headaches
Preventing headache symptoms from allergies requires sustained allergen avoidance combined with pre-emptive treatment before allergy season peaks.
Key prevention steps:
- Start nasal corticosteroid sprays 2 weeks before your local pollen season begins, since they require time to reach full anti-inflammatory effect.
- Check daily pollen counts on the National Allergy Bureau website and limit outdoor activity when counts exceed moderate levels (50–499 grains per cubic meter for trees, 25–499 for grass).
- Replace HVAC air filters every 30 days during allergy season with MERV 13-rated filters.
- Wash bedding weekly in water above 130°F to kill dust mites, reducing year-round allergen load.
- Avoid known food cross-reactants during pollen season. Birch pollen allergic patients often react to apples, peaches, and almonds through oral allergy syndrome, which amplifies nasal inflammation.
- Complete immunotherapy before high-exposure seasons for maximum protection.
FAQs
1. Can allergies cause headaches every day?
Yes, allergies can cause headaches daily when allergen exposure is continuous, as with dust mite allergy or mold. Daily perennial allergic rhinitis produces ongoing sinus congestion and pressure pain without seasonal breaks. Untreated, it can persist year-round.
2. Can seasonal allergies trigger headaches?
Yes, seasonal allergies trigger headaches through histamine-driven nasal swelling that blocks sinus drainage. Ragweed season (August to October) produces the highest headache burden. Pollen counts above 500 grains per cubic meter correlate directly with increased sinus headache reports.
3. What do allergy headaches feel like?
Headache symptoms from allergies feel like constant dull pressure across the forehead, cheeks, or around the eyes. The pain does not throb. It worsens when bending forward. Facial tenderness on tapping the sinus areas confirms the source.
4. How does sinus inflammation cause headaches?
Sinus inflammation causing headaches works through blocked drainage. Swollen sinus mucosa seals the drainage openings. Trapped air creates 10–30 mmHg negative pressure inside the sinus cavity. This negative pressure pulls against sinus walls, producing deep, aching pain.
5. Can nasal congestion and pressure cause head pain?
Yes. Nasal congestion and pressure headaches develop within minutes of acute sinus blockage. Blocked drainage channels allow pressure differentials to build across sinus walls. The frontal and maxillary sinuses produce the most noticeable pain when blocked.
6. Are allergy headaches different from migraines?
Yes. Allergy headaches produce constant, non-pulsating pressure with active nasal symptoms. Migraines produce pulsating pain that worsens with activity, with nausea and light sensitivity. However, allergic rhinitis triggers migraines 5.6x more often in susceptible patients (Martin et al., Cephalalgia, 2016).
7. Which allergens are most likely to trigger headaches?
Ragweed is the most common outdoor trigger in the USA, affecting 23 million people. Dust mites cause the most year-round nasal congestion and pressure headaches indoors. Pet dander (Fel d 1 from cats) stays airborne longest and triggers the most sustained sinus pressure.
8. Can pollen allergies cause headaches?
Yes. Allergies can cause headaches from pollen: tree pollen triggers frontal sinus pain; grass pollen triggers diffuse facial pressure; ragweed pollen triggers the most intense sinus response due to particle size and potency. Pollen headaches resolve within hours of leaving high-exposure environments.
9. How can I relieve allergy headaches naturally?
How to relieve allergy headaches without medication: saline nasal irrigation flushes allergens and thins mucus; sleeping at 30–45 degrees improves drainage; warm compresses on sinuses reduce wall tension; staying hydrated keeps mucus thin. These methods reduce headache intensity within 30–60 minutes.
10. What medications help allergy-related headaches?
Nasal corticosteroid sprays (fluticasone, mometasone) are the most effective for sinus inflammation causing headaches with daily use. Oral pseudoephedrine decongest faster for acute relief. Ibuprofen 400mg reduces both sinus inflammation and headache pain simultaneously and is the preferred analgesic for allergy headaches.
References
- Asthma and Allergy Foundation of America (AAFA), Ragweed Season Data
- American Academy of Allergy, Asthma and Immunology (AAAAI), Immunotherapy Guidelines
- National Allergy Bureau, Pollen Count Data
- Martin VT et al. Cephalalgia, 2016. Allergic Rhinitis and Migraine Frequency
- Kimoto K et al. International Journal of Biometeorology, 2011. Barometric Pressure and Sinus Headache
- Cochrane Review, Saline Nasal Irrigation for Allergic Rhinitis, 2007
- U.S. Food and Drug Administration, Dupilumab Approval for Chronic Rhinosinusitis with Nasal Polyps, 2019
- Clinical and Experimental Allergy, Cognitive Impairment Meta-analysis, 2018