
The stages of liver fibrosis range from F0 (no scarring) to F4 (cirrhosis). Each stage reflects how much scar tissue has built up from ongoing liver injury. Early stages can reverse with treatment. Stage F4 is largely permanent and requires lifelong medical management.
Over 4.5 million adults in the US live with chronic liver disease, according to the CDC. Most have fibrosis forming silently for years before a diagnosis. This guide covers causes, what each stage means, warning signs, and the current evidence on reversibility.
How Liver Fibrosis Develops Over Time
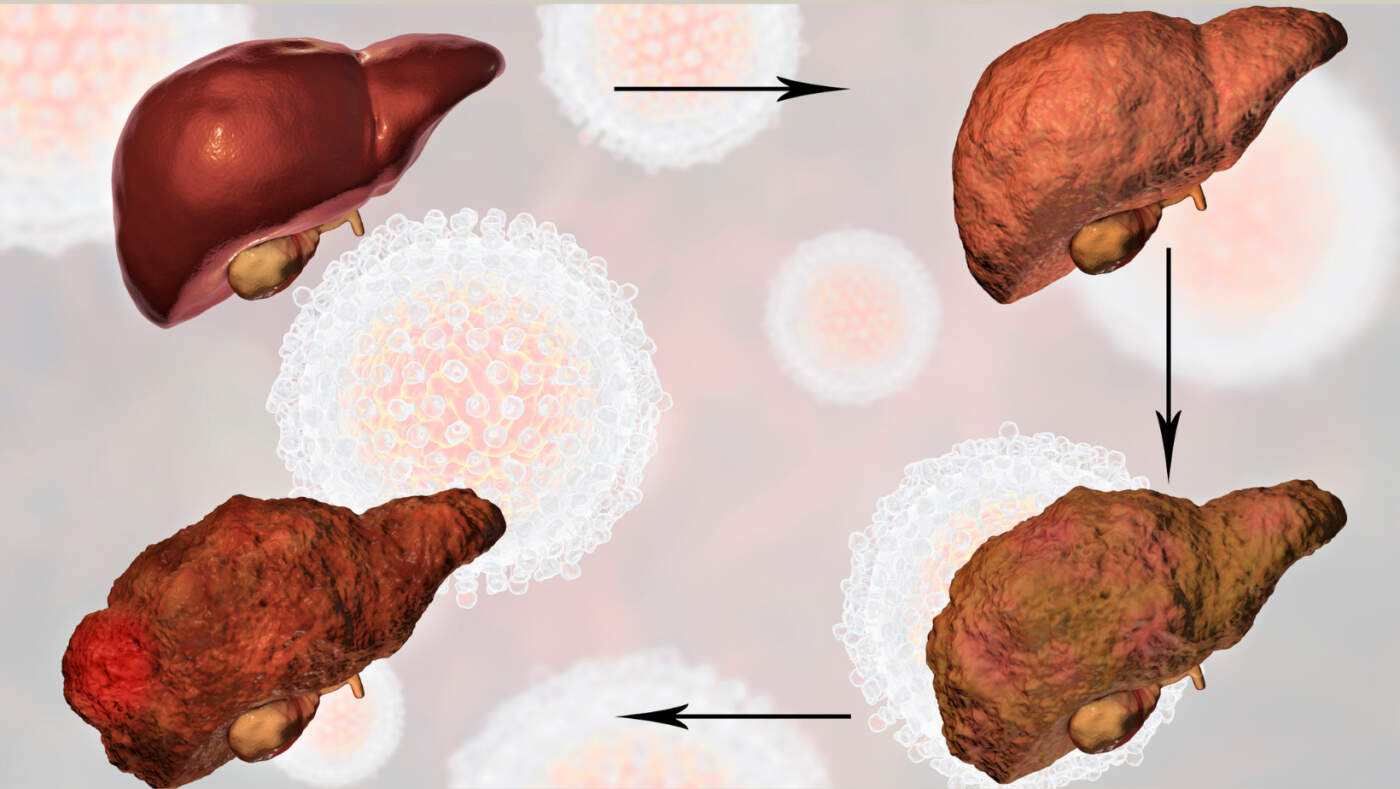
How liver fibrosis develops over time follows a predictable biological chain: repeated injury triggers inflammation, which activates scar-producing cells, which lay down collagen. Left unchecked, that collagen builds into fibrosis.
Chronic Inflammation and Liver Injury
Every liver injury triggers inflammation as a healing response. When damage stops, inflammation clears and the liver repairs itself. When damage is ongoing, whether from alcohol, fat, or a virus, inflammation becomes chronic and starts fibrosis.
Activation of Scar-Producing Cells
Chronic inflammation activates hepatic stellate cells. These cells stay dormant in a healthy liver. Once activated, they produce collagen. Excess collagen forms fibrous bands that replace healthy liver tissue.
Progressive Accumulation of Scar Tissue
Collagen builds up around the liver’s blood vessels and bile ducts. Early on, the liver compensates. Over years, scar tissue thickens and spreads, disrupting the liver’s internal structure.
Loss of Healthy Liver Function
Healthy liver cells, called hepatocytes, filter toxins, produce proteins, and store energy. As scar tissue expands, fewer functional hepatocytes survive. Liver function declines in proportion to how much scarring exists.
Transition Toward Cirrhosis
At advanced fibrosis, the liver’s normal structure gets replaced by nodules of surviving cells surrounded by thick scar bands. This is the defining pattern of cirrhosis. Blood flow through the liver becomes restricted, raising pressure in surrounding vessels.
Common Causes of Liver Fibrosis
Multiple conditions trigger the same chain of inflammation, stellate cell activation, and collagen buildup.
Fatty Liver Disease (MASLD)
Metabolically-dysfunction-associated steatotic liver disease (MASLD, formerly NAFLD) is now the leading cause of liver fibrosis in the US. A 2023 analysis in Hepatology estimated that roughly 38% of US adults have fatty liver. Fat deposits in liver cells cause low-grade inflammation that, over years, drives scarring.
Alcohol-Related Liver Disease
Heavy alcohol use directly injures liver cells and fuels inflammation. Fibrosis from alcohol progresses faster than from fatty liver, especially with heavy daily drinking lasting more than 10 years.
Chronic Hepatitis B
Hepatitis B embeds itself in liver cell DNA. The immune system continuously attacks infected cells. That immune response, not the virus itself, drives ongoing fibrosis.
Chronic Hepatitis C
Before effective antivirals, hepatitis C was the top reason for liver transplants in the US. Decades of viral replication trigger sustained inflammation. Current direct-acting antivirals cure over 95% of cases, but existing scarring remains.
Autoimmune Liver Disorders
In autoimmune hepatitis, primary biliary cholangitis (PBC), and primary sclerosing cholangitis (PSC), the immune system attacks liver cells or bile ducts directly. These require long-term immunosuppressive or targeted therapy to slow fibrosis progression.
Metabolic and Genetic Conditions
Hemochromatosis (iron overload), Wilson disease (copper accumulation), and alpha-1 antitrypsin deficiency each cause fibrosis through distinct toxicity mechanisms. These are less common but frequently missed during standard workups.
Liver Fibrosis Stages Explained
The stages of liver fibrosis use the METAVIR scoring system, developed for liver biopsy interpretation. Scores run from F0 to F4.
| METAVIR Stage | Description | Reversibility |
| F0 | No fibrosis | N/A |
| F1 | Mild fibrosis | Yes, with treatment |
| F2 | Moderate fibrosis | Partially reversible |
| F3 | Advanced fibrosis | Difficult but possible |
| F4 | Cirrhosis | Mostly irreversible |
Stage F0: No Fibrosis
At F0, no scar tissue exists. Liver architecture is intact. Having a cause of liver injury, such as obesity, heavy alcohol use, or hepatitis B or C, without yet showing fibrosis still places someone at elevated risk. Prevention works best here. Weight loss of 5 to 10% in people with fatty liver reduces liver fat measurably. Antiviral treatment for hepatitis B or C prevents fibrosis from ever starting.
Stage F1: Mild Liver Fibrosis
Liver fibrosis stages at F1 show early collagen deposits around the portal tracts, the areas where blood vessels and bile ducts enter the liver. This change is microscopic with no outward symptoms. Blood tests like ALT and AST may be mildly elevated but often read within a borderline-normal range.
Early Scar Tissue Formation
Scar tissue at F1 is confined and minimal. It does not yet disrupt blood flow or impair liver function measurably. This stage is frequently detected only through FibroScan, MRI elastography, or biopsy done for an unrelated reason.
Importance of Early Lifestyle Changes
F1 is the stage where intervention has the greatest impact. A 2021 study in the Journal of Hepatology found that sustained weight loss of 7 to 10% reversed F1 fibrosis in a meaningful proportion of MASLD patients within 12 months. This is the window where the liver still responds readily.
Stage F2: Moderate Liver Fibrosis
At F2, fibrosis has extended beyond the portal tracts and begun forming bridges between different structural zones. The stages of liver fibrosis become clinically significant here. Portal-to-portal bridging fibrosis defines this stage. More collagen means more structural disruption. The liver’s regenerative capacity starts to show strain.
Some people at F2 notice mild fatigue or upper right abdominal discomfort. These symptoms alone cannot diagnose fibrosis. A FibroScan result between 7.0 and 9.5 kPa typically corresponds to F2 in most liver disease types, though cutoffs vary by condition.
Stage F3: Advanced Liver Fibrosis
F3 is where clinical risk rises sharply. Multiple fibrous bridges now cross the liver in several directions. Normal lobular structure is distorted but not yet replaced by regenerative nodules. That distinction separates F3 from cirrhosis.
A healthy liver reads below 5 kPa on FibroScan. At F3, readings typically fall between 9.5 and 12.5 kPa. Without treatment, the annual progression rate from F3 to F4 in active hepatitis C is estimated at 10 to 20% per year. F3 is the last stage where serious regression is still achievable.
Gastroenterology or hepatology referral is standard at F3. Surveillance for esophageal varices begins. Liver cancer screening with ultrasound every six months becomes recommended at some centers even before full cirrhosis develops.
Stage F4: Cirrhosis
F4 marks cirrhosis. The entire liver architecture reorganizes around regenerative nodules encased in thick scar bands. Blood cannot move through normally.
The liver loses the ability to produce adequate clotting factors, albumin, and bile. Toxin removal slows. Bilirubin accumulates. Ammonia builds up and can impair brain function. Decompensated cirrhosis, when the liver can no longer maintain basic function, presents with ascites (fluid in the abdomen), hepatic encephalopathy (confusion from ammonia), and variceal bleeding.
Long-term complications at F4 include:
- Hepatocellular carcinoma risk of 1 to 4% per year
- Portal hypertension and variceal bleeding
- Spontaneous bacterial peritonitis
- Hepatorenal syndrome (kidney failure secondary to liver failure)
- Liver transplant evaluation
Advanced Liver Fibrosis Signs
Advanced liver fibrosis signs in people with F3, or even early F4, feel reasonably well until something breaks through.
Persistent Fatigue
This is not ordinary tiredness. It does not improve with sleep. It comes from impaired energy metabolism when the liver cannot efficiently process nutrients and clear toxins.
Abdominal Discomfort
A dull pressure in the upper right abdomen can reflect liver enlargement or tension from portal hypertension. Most people describe it as fullness rather than sharp pain.
Unexplained Weight Loss
Muscle wasting in advanced fibrosis comes from the liver’s reduced ability to synthesize proteins. Weight loss with muscle loss, despite eating normally, is a warning sign.
Easy Bruising
The liver produces clotting factors. When it cannot make enough, minor bumps leave large bruises. This is often what brings people to their doctor first.
Swelling in the Legs or Abdomen
Reduced albumin production causes fluid to leak into the surrounding tissue. Leg swelling is common. Ascites (fluid pooling in the abdomen) signals decompensated cirrhosis.
Jaundice
Yellowing of the skin and eyes occurs when bilirubin cannot be processed by a failing liver. Jaundice at this level requires urgent medical evaluation.
Can Liver Fibrosis Be Reversed?
Liver fibrosis can be reversed at stages F1 and F2. Partially, at F3. Rarely at F4.
Reversibility of Early-Stage Fibrosis
F1 and F2 fibrosis can fully reverse with sustained treatment of the underlying cause. The liver’s ability to break down excess collagen through enzymes called matrix metalloproteinases remains active at these stages. Remove the trigger, and the liver starts cleaning up.
Addressing the Underlying Cause
In hepatitis C, cure means achieving a sustained virologic response (SVR) with antiviral medications. In MASLD, it requires metabolic improvement through weight loss and blood sugar control. In alcohol-related fibrosis, abstinence is the primary intervention.
Role of Lifestyle Changes
A 2023 clinical review in Gastroenterology confirmed that 7 to 10% body weight reduction in MASLD patients was associated with fibrosis regression across multiple studies. Exercise independently improved liver stiffness scores even without significant weight loss.
Limits of Reversal in Advanced Disease
At F4, cirrhosis rarely reverses fully. Some studies have documented partial regression after hepatitis C cure. But the structural nodular pattern typically remains. The focus at F4 shifts to preventing decompensation, managing complications, and evaluating transplant eligibility. Liver fibrosis cannot be reversed fully at this stage.
FAQs
What is the difference between liver fibrosis and cirrhosis?
Fibrosis (F1 to F3) is scar buildup that has not yet destroyed the liver’s internal structure. Cirrhosis (F4) means the liver has reorganized around nodules of surviving cells encased in scar. Cirrhosis carries permanent complication risks that earlier fibrosis stages do not.
What is a FibroScan?
FibroScan uses ultrasound to measure liver stiffness in kilopascals. Below 5 kPa is normal. Above 12.5 kPa suggests cirrhosis in most conditions. The test takes under 10 minutes, requires no needles, and correlates closely with biopsy findings.
Can fatty liver disease lead to fibrosis?
Yes. MASLD progresses to fibrosis in 20 to 30% of patients over 10 to 20 years. Those with diabetes, obesity, and elevated liver enzymes progress fastest. Most with simple fatty liver never reach cirrhosis, but fibrosis at F3 or F4 usually has no symptoms until complications appear.
What treatments are available for liver fibrosis?
Treatment options for liver fibrosis depend on the cause: direct-acting antivirals for hepatitis C, tenofovir or entecavir for hepatitis B, weight loss and metabolic control for MASLD, and corticosteroids or ursodeoxycholic acid for autoimmune disease. Resmetirom, FDA-approved in March 2024, showed fibrosis regression in F2 to F3 MASLD patients in the MAESTRO-NASH trial.
Can liver fibrosis progress to liver cancer?
Yes. At F4, hepatocellular carcinoma develops in 1 to 4% of patients per year. Risk exists at F3, especially with chronic hepatitis B. Ultrasound screening every 6 months is standard at cirrhosis and recommended at F3 in high-risk patients.
How quickly does liver fibrosis progress?
Hepatitis C advances roughly one METAVIR stage every 7 to 10 years on average, but 20% of patients progress faster. Alcohol-related fibrosis moves faster with daily heavy drinking. MASLD is slower but accelerates sharply with diabetes or severe obesity. Some patients go from F1 to F4 in under a decade.
Sources
- American Liver Foundation – Liver Fibrosis
- NIDDK – Cirrhosis Overview
- CDC – Chronic Liver Disease Statistics
- Hepatology (2023) – MASLD Prevalence in US Adults
- Journal of Hepatology (2021) – Weight Loss and Fibrosis Regression
- Gastroenterology (2023) – Lifestyle Interventions and Fibrosis Regression
- NEJM (2024) – MAESTRO-NASH Trial: Resmetirom for MASH
- AASLD – MASLD Practice Guidelines
- Mayo Clinic – Cirrhosis: Symptoms and Causes
- WHO – Hepatitis B and C Fact Sheets










Leave a Comment