COPD affects over 300 million people worldwide, and most of them don’t know they have it until it’s already Stage 2 or beyond. The earliest symptoms are easy to miss. You can’t diagnose COPD at home. But you can spot warning signs early enough to act before real damage builds up.
Testingyourself for COPD at home gives you enough information to act before the disease advances. A 20-minute spirometry test at your GP clinic changes everything when it detects and this is the Stage at COPD.
Early Signs of COPD Self-Assessment
Early signs of COPD self-assessment starts with paying attention to patterns. A daily cough for three months straight means something.
Persistent Cough Patterns to Notice
A COPD-related cough isn’t occasional. It shows up most mornings. It produces mucus. It doesn’t fully clear after a few days the way a cold does. If you’ve been coughing 8 or more weeks with no clear cause, that’s a pattern worth tracking and reporting to a doctor.
Daily Mucus Production Signals
Healthy lungs produce mucus. COPD lungs produce too much mucus. Regularly coughing up mucus in the morning before engaging in any physical activity indicates inflammation in your airways. Yellow or green mucus means active infection.
Breathlessness During Simple Activities
Getting winded climbing one flight of stairs is not normal at any age under 70. Experiencing breathlessness while dressing or speaking full sentences is a significant warning sign. COPD breathlessness doesn’t come on suddenly. It creeps up slowly over months.
Wheezing and Chest Tightness Clues
Wheezing is a high-pitched whistling sound when you breathe out. It happens when airways narrow. Chest tightness without a cardiac cause points to airway obstruction. Both can occur in asthma too, so the full picture matters.
Can You Check COPD at Home
You can screen yourself for COPD symptoms and track risk factors. You cannot confirm COPD without spirometry. A self-check tells you whether to seek medical testing. It doesn’t replace that testing.
What Self-Testing Can and Cannot Confirm
Self-testing confirms symptom presence. It tracks breathlessness severity. It monitors oxygen levels with a pulse oximeter. It cannot measure FEV1 or FVC, the two numbers that actually confirm COPD through spirometry. Home checks are screening tools, not diagnostic tools.
Difference Between Screening vs Diagnosis
Screening means identifying people at risk who need further testing. Diagnosis means confirming the disease using clinical measurements. You can screen to test yourself for COPD at home. A pulmonologist diagnoses it with spirometry.
When Home Checks Are Useful
Home checks are most useful for people over 40 who smoke or have smoked, people with regular cough or breathlessness, and anyone with a family history of early lung disease. If you fall into these groups, systematic self-monitoring gives your doctor better data to work with.
Limitations You Must Understand
Home checks miss early-stage COPD completely. At Stage 1, symptoms are subtle and oxygen levels remain normal. Most people who check themselves feel “fine” but have already lost 20% of lung function. This is why spirometry for high-risk individuals over 40 is recommended annually by GOLD guidelines.
Shortness of Breath COPD Self-Check
Shortness of breath COPD self-check methods give you a practical, repeatable way to monitor your breathing capacity over weeks and months.
6-Minute Walk Self-Test Method
Walk at your normal pace for 6 minutes on flat ground. Measure the distance. Healthy adults over 40 cover 400–700 meters. If you cover less than 350 meters or need to stop due to breathlessness, that’s below the expected range for your age group. Repeat monthly and track changes.
Stair Test for Breath Capacity
Walk up two flights of stairs at a comfortable pace without stopping. If you feel significant breathlessness before reaching the top, or if you need more than 2 minutes to recover afterward, your breathing capacity warrants medical evaluation.
Talking Test (Speech Limitation Check)
Read a paragraph aloud at normal speaking pace. Healthy breathing lets you speak 20–25 words before needing a breath. If you need to pause every 8–10 words or feel breathless after one sentence, your breathing is restricted beyond normal.
Tracking Breathlessness Over Time
Use the Modified Medical Research Council (MRC) dyspnea scale. It runs from Grade 0 (no breathlessness except heavy exercise) to Grade 4 (too breathless to leave the house). Track your grade weekly. Progression by even one grade over 3 months means your breathing is worsening and needs clinical review.
Home Pulse Oximeter for COPD Monitoring
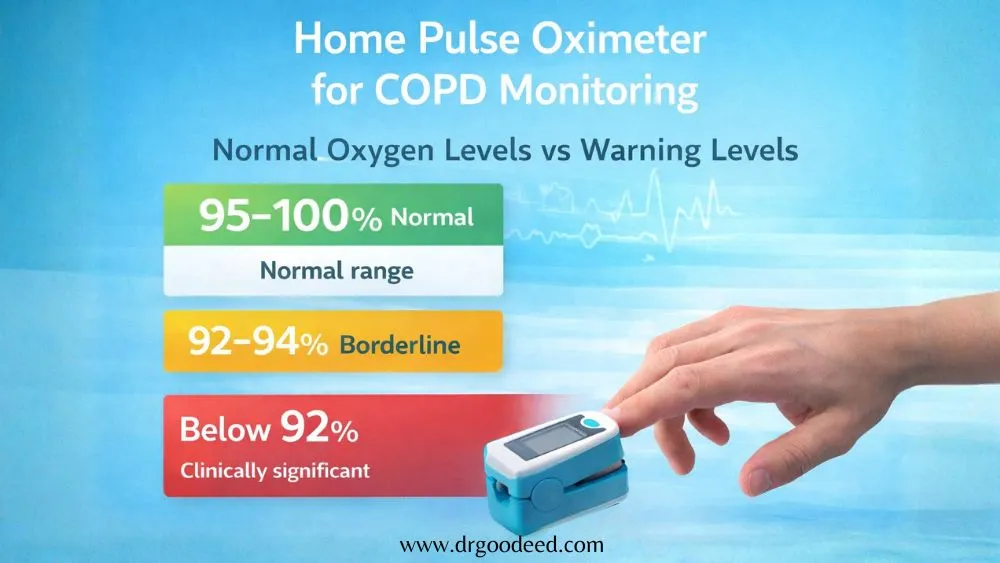
Home pulse oximeter for COPD monitoring is one of the most practical tools available to patients. A basic fingertip oximeter costs under $25 and gives you real-time oxygen saturation data.
Normal Oxygen Levels vs Warning Levels
- 95–100%: Normal range for healthy adults
- 92–94%: Borderline low; warrants monitoring and medical discussion
- Below 92%: Clinically significant; consult a doctor within 24 hours
- Below 88% at rest: Threshold for long-term oxygen therapy prescription
How to Correctly Use a Pulse Oximeter
Warm your hands before testing. Cold fingers cause falsely low readings. Sit still for 5 minutes. Place the device on your middle or index finger. Wait 30 seconds for a stable reading. Test in the morning before activity and after walking up stairs. Both readings give different information.
When Low Oxygen Becomes Dangerous
Sustained SpO2 below 88% at rest causes strain on the right side of the heart, a condition called cor pulmonale. Levels below 85% during sleep can cause morning headaches, confusion, and cardiac arrhythmias. One low reading isn’t an emergency. Consistently low readings across multiple days are.
Common Mistakes in Readings
Nail polish, especially dark colors, blocks the sensor and gives falsely low readings. Moving the finger during measurement causes errors. Poor circulation from Raynaud’s disease also affects accuracy. If your reading seems too low, check again on a different finger and ensure the probe fits snugly.
Simple COPD Self-Test Questionnaire
The COPD Assessment Test (CAT) is a validated 8-question tool used globally. You can find it free at copdassessmenttest.com. It measures cough frequency, mucus, chest tightness, breathlessness, activity limitation, confidence leaving home, sleep quality, and energy levels. Scores above 10 indicate significant disease impact and warrant medical review.
Use it to test yourself for COPD impact, not to confirm diagnosis. Answer these questions honestly:
- Do you cough daily, even when you’re not sick?
- Do you produce mucus every morning?
- Does your chest feel tight regularly?
- Do you get breathless doing tasks you managed easily 2 years ago?
- Do you wake up at night due to breathing discomfort?
- Does breathlessness stop you from doing activities you want to do?
Three or more “yes” answers in someone over 40 with any smoking or pollution history means spirometry testing is appropriate.
Risk Factors That Increase COPD Chances
Early signs of COPD self-assessment only makes sense in the context of risk. Without risk factors, many symptoms point to other conditions. With significant risk factors, even mild symptoms warrant investigation.
Smoking and Secondhand Smoke Exposure
Smoking causes 70–80% of COPD cases. One pack a day for 20 years (20 pack-years) puts you in a high-risk category. But secondhand smoke exposure at home for 10 or more years also causes COPD in non-smokers, especially during childhood.
Air Pollution and Occupational Hazards
Biomass fuel smoke from wood-burning stoves is the leading COPD cause in non-smoking women in South Asia and Sub-Saharan Africa. Occupational dust from coal mining, grain handling, and textile manufacturing causes COPD in non-smokers at similar rates to light smokers.
Recurrent Respiratory Infections
Severe pneumonia in childhood permanently reduces maximum lung capacity. Adults who had three or more chest infections per year during childhood carry a measurably higher COPD risk by age 40, regardless of smoking history.
Family History of Lung Disease
A family history of early-onset emphysema (before age 50) or unexplained COPD in a non-smoker points to a genetic risk worth investigating. Genetic COPD runs in families but often goes undiagnosed for generations.
Genetic Risk Alpha-1 Antitrypsin COPD
Genetic risk alpha-1 antitrypsin COPD is the most underdiagnosed cause of lung disease in younger adults. Most doctors don’t test for it unless prompted.
What Is Alpha-1 Antitrypsin Deficiency
Alpha-1 antitrypsin (AAT) is a protein made in the liver that protects lung tissue from immune-cell damage. People with AAT deficiency produce little or none of it. Their lungs break down significantly faster. COPD develops in their 40s instead of their 60s.
Why COPD Occurs in Non-Smokers
Genetic risk alpha-1 antitrypsin COPD explains why some non-smokers develop severe emphysema young. Without AAT protecting lung tissue, even normal breathing and minor infections cause progressive alveolar destruction.
Who Should Consider Genetic Testing
- Anyone diagnosed with COPD before age 50
- Non-smokers with confirmed COPD
- Anyone with a first-degree relative with early-onset emphysema
- COPD patients whose disease progresses faster than expected despite treatment
GOLD guidelines recommend one-time AAT blood testing for all COPD patients.
Early Detection Importance
People with AAT deficiency qualify for AAT augmentation therapy, weekly intravenous infusions of the missing protein. Alpha-1 Foundation data shows augmentation therapy slows CT-measured emphysema progression by 34% compared to placebo. Early detection makes this intervention possible.
When Home Testing Is Not Enough
Home monitoring tracks symptoms. It doesn’t catch disease before symptoms start, and it misses acute deterioration that needs urgent care.
Warning Symptoms Needing Medical Help
Seek same-day medical attention for:
- Breathlessness that worsens suddenly over hours
- A cough producing blood, even a small amount
- Fever above 38.5°C with increased mucus and breathlessness
- Chest pain with any breathing difficulty
Sudden Worsening Breathlessness
Sudden severe breathlessness in a COPD patient signals an exacerbation, pneumonia, pulmonary embolism, or pneumothorax. None of these wait. A rescue inhaler that isn’t working after 10–15 minutes means go to an emergency room.
Blue Lips or Low Oxygen Signs
Blue or gray coloring on lips, fingernails, or around the mouth is cyanosis. It means oxygen in your blood has dropped below safe levels. This is an emergency. Call for an ambulance immediately.
Frequent Chest Infections
More than two chest infections requiring antibiotics per year in a COPD patient means the disease is inadequately controlled. Each infection permanently worsens lung function. This pattern needs specialist review, not just repeat antibiotic courses.
Medical Tests Doctors Use for COPD
Spirometry (Gold Standard Test)
Spirometry measures FEV1 (air forced out in one second) and FVC (total air breathed out). An FEV1/FVC ratio below 0.70 after a bronchodilator confirms COPD. No other test replaces this. It takes 20 minutes and is available at most GP clinics.
Chest X-Ray and CT Scan Role
Chest X-rays show hyperinflation and bullae (large air pockets) in advanced COPD. They miss early disease entirely. High-resolution CT scans detect emphysema at Stage 1, before spirometry confirms obstruction. Low-dose CT is now included in lung cancer screening programs in the U.S., which incidentally catches early COPD.
Arterial Blood Gas Testing
Arterial blood gas (ABG) testing measures oxygen and carbon dioxide levels directly in the blood. It’s used in Stage 3 and 4 COPD to assess respiratory failure risk and guide oxygen therapy decisions. It requires a blood draw from the wrist artery, not a standard vein.
Lung Function Grading
After spirometry, doctors use the GOLD 1–4 staging system based on FEV1 percentage to grade severity. They also assess symptom burden using the CAT score and exacerbation history to assign a severity group (A, B, or E). Both inform treatment decisions.
Can COPD Be Detected Early
Yes. But it requires actively looking for it in high-risk people, not waiting for them to report severe symptoms. Early detection changes outcomes.
Why Early Stages Go Unnoticed
At Stage 1, FEV1 is above 80%. Symptoms are minimal. Most patients write off morning cough as smoking-related or normal. The average delay between first symptoms and diagnosis is 4–7 years, based on a 2021 Lancet Respiratory Medicine analysis.
Importance of Symptom Tracking
Writing down breathlessness episodes, cough frequency, and mucus production weekly gives a doctor useful longitudinal data. A single clinic visit captures one moment. Months of self-tracked data reveals the trend.
Screening High-Risk Individuals
You can check COPD at home as part of a screening program. The CAPTURE questionnaire (a 5-question tool developed specifically for COPD primary care screening) has 88% sensitivity for detecting undiagnosed COPD. It’s free and takes under 2 minutes.
Preventing Disease Progression
Quitting smoking at Stage 1 reduces FEV1 decline to near-normal aging rates within 5 years. Annual spirometry for high-risk adults over 40 catches disease before symptoms become disabling. Acting at Stage 1 gives patients 15–20 more years of preserved lung function.
Frequently Asked Questions
What is the first sign of COPD?
A productive morning cough lasting more than 8 weeks is the first clinical sign in most patients. It appears years before breathlessness. Most people dismiss it as a smoker’s cough. That delay is why 70% of COPD cases are diagnosed late.
How do I know if my breathlessness is serious?
Breathlessness that stops you from completing one flight of stairs without pausing is medically significant. Use the MRC dyspnea scale. Grade 2 or above (breathless on level ground at your own pace) warrants spirometry testing regardless of age.
What oxygen level is dangerous?
SpO2 below 92% warrants same-day medical contact. Below 88% at rest is the clinical threshold for prescribing long-term oxygen therapy. Below 85% during sleep causes cardiac arrhythmias and right heart strain. One reading below 88% on a warm, still finger needs clinical follow-up within 24 hours.
Is a pulse oximeter enough to detect COPD?
No. A pulse oximeter measures oxygen saturation, not airflow obstruction. COPD patients maintain normal SpO2 well into Stage 2 and sometimes Stage 3. A normal oximeter reading does not rule out COPD. Spirometry is the only test that confirms it.
Can non-smokers get COPD?
Yes. Approximately 25% of COPD patients never smoked. Genetic risk alpha-1 antitrypsin COPD, biomass fuel exposure, occupational dust, and childhood respiratory infections all cause COPD without any cigarette use. Non-smokers with breathlessness deserve spirometry evaluation, not reassurance based on their non-smoking status.
How accurate are online COPD tests?
Online symptom questionnaires like the CAT and CAPTURE tool have 80–88% sensitivity for detecting undiagnosed COPD in high-risk adults. They are not diagnostic. They identify who needs spirometry. Using them to test yourself for COPD risk is reasonable; treating them as a diagnosis is not.
When should I see a doctor for COPD symptoms?
See a doctor within 2 weeks if you have daily cough with mucus, breathlessness on mild exertion, or wheeze for more than 4 weeks. See a doctor same-day if your rescue inhaler stops working, mucus turns green with fever, or SpO2 drops below 92%.
Can COPD be reversed if caught early?
No. Structural damage is permanent. But shortness of breath COPD self-check results improve significantly after early diagnosis and smoking cessation. Stage 1 patients who quit smoking reduce annual FEV1 decline by 50–60%, effectively preserving lung function for decades.
What is the best test to confirm COPD?
Spirometry with a post-bronchodilator FEV1/FVC ratio below 0.70 is the only test that confirms COPD. High-resolution CT adds detail about the extent. Blood testing for AAT deficiency should accompany diagnosis in all patients per GOLD guidelines.