
COPD is classified into four stages based on the degree of airflow obstruction in your lungs. Stage 1 is mild. Stage 4 is life-limiting. Each stage needs a different treatment approach.
A Stage 1 diagnosis with immediate action preserves years of functional life. Even at Stage 4, treatment adherence changes survival odds. Getting spirometry done early is the one step that changes everything.
How COPD Is Classified Into Stages
COPD is classified into stages according to a system called GOLD, developed by the Global Initiative for Chronic Obstructive Lung Disease. It uses a breathing test called spirometry to measure how much air you can force out in one second. That number, FEV1, tells doctors how damaged your lungs are.
GOLD Staging System Explained
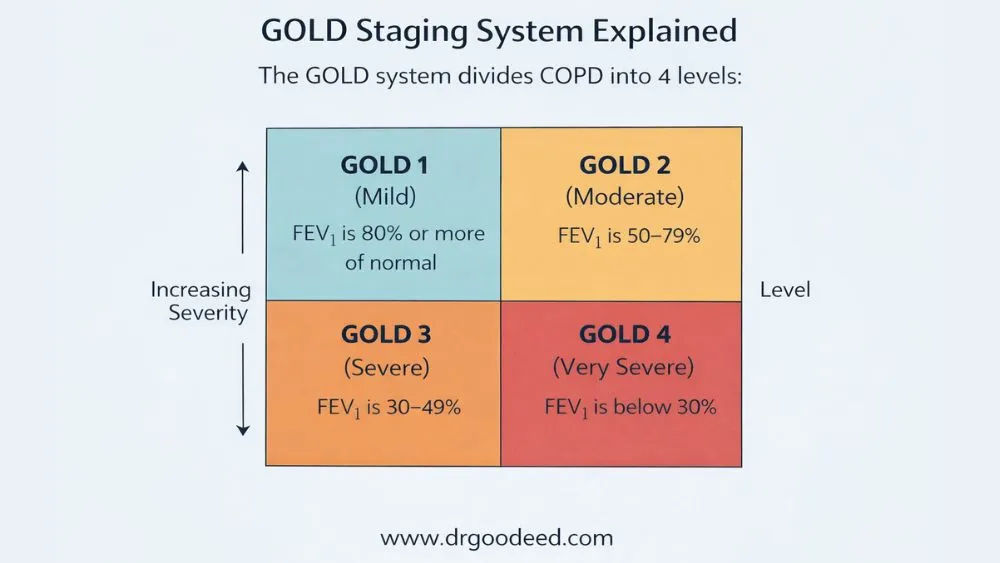
The GOLD system divides COPD into 4 levels:
- GOLD 1 (Mild): FEV1 is 80% or more of normal
- GOLD 2 (Moderate): FEV1 is 50–79%
- GOLD 3 (Severe): FEV1 is 30–49%
- GOLD 4 (Very Severe): FEV1 is below 30%
Role of Spirometry (FEV1 Measurement)
Spirometry is the only test that confirms COPD. You breathe hard into a machine. If the FEV1/FVC ratio is below 0.70 after a bronchodilator, COPD is confirmed. FVC is the total air you can breathe out in one go. This ratio is fixed. It doesn’t lie.
Difference Between Stages vs Severity Groups
Stages 1–4 measure lung function. Severity groups (A, B, C, D) measure your symptom burden and flare-up history. A patient can be GOLD 2 by FEV1 but Group D by symptoms. Doctors use both to build a treatment plan.
Why Staging Matters for Treatment Decisions
A Stage 1 patient needs a short-acting inhaler on bad days. A Stage 4 patient needs 24-hour oxygen, multiple inhalers, and sometimes surgery. Same disease. Very different treatment. Staging removes the guesswork.
Lung Damage and Airflow Limitation Stages
The lung damage and airflow limitation stages are not the same thing. Airflow limitation is what a test measures. Lung damage is what’s happening inside. Both occur together, but damage usually runs ahead of symptoms.
What Happens Inside the Lungs in COPD
Your lungs have millions of tiny air sacs called alveoli. COPD destroys them slowly. It also inflames and narrows airways. The result: air gets trapped inside, carbon dioxide builds up, and oxygen drops. Breathing gets harder every year.
Airflow Obstruction and Inflammation
The inflammation in COPD is not like a cold. It’s chronic. Neutrophils and macrophages, two immune cell types, stay active in your lungs even when you feel fine. They release chemicals that eat away at lung tissue over months. Smoking speeds this up. Quitting slows it. But it doesn’t reverse existing damage.
Structural Damage in Early vs Late Stages
In early COPD, small airways narrow. If you remove irritant exposure early enough, this is partly reversible. By Stage 3, alveoli are destroyed, and the walls between them collapse. This is emphysema. No medication rebuilds those walls.
Irreversible vs Manageable Changes
Airway inflammation responds to steroids and bronchodilators. Alveolar destruction does not. This is why catching COPD early changes long-term outcomes.
Stage 1 COPD: Early Changes You Might Miss
Stage 1 is where most diagnoses fail to happen. FEV1 is above 80%, symptoms are mild, and most people blame the cough on smoking or seasonal allergies. Lung damage is already underway.
Mild Airflow Limitation Explained
The lungs work at 80% or more capacity. That sounds fine. But the 20% loss already causes micro-damage to small airways. Breathlessness at rest is absent. Heavy exertion triggers mild discomfort.
Subtle Symptoms Often Ignored
- A mild morning cough that clears mucus
- Slightly longer recovery after physical activity
- Occasional wheezing, especially in cold air
- Fatigue after tasks that used to feel normal
Most people ignore these for years.
Risk Factors
Smoking is the biggest risk. But long-term exposure to coal dust, grain dust, or chemical fumes also causes COPD in non-smokers. Severe childhood pneumonia increases risk decades later.
Early Intervention Strategies
Quitting smoking at Stage 1 can bring FEV1 decline close to normal aging rates. GOLD recommends annual spirometry for people over 40 who smoke. Pulmonary rehab at this stage is underused but genuinely effective.
Stage 2 COPD: Symptoms Start Affecting Daily Life
FEV1 drops to 50–79%. This is when most patients finally see a doctor. Symptoms are no longer subtle.
Worsening Breathlessness Patterns
Breathlessness during exertion becomes consistent. Walking upstairs or carrying groceries triggers it. It’s not just fitness decline. The lungs are working harder than they should for basic activity.
Chronic Cough and Mucus Production
The cough becomes daily. Mucus production increases because inflamed airways trigger mucus glands to overwork. Some patients cough up mucus every morning for years before getting diagnosed.
Impact on Physical Activity
Exercise tolerance drops noticeably. Someone who walked 2 miles easily now struggles with one. Reduced activity weakens muscles, which makes breathlessness worse. It becomes a reinforcing loop.
When Patients Usually Get Diagnosed
Most COPD diagnoses happen at Stage 2. A 2021 Lancet study showed the average delay between first symptoms and diagnosis is 4–7 years. Earlier spirometry screening changes this outcome significantly.
Stage 3 COPD: Severe Airflow Limitation
FEV1 is now 30–49%. Daily life is heavily restricted. COPD shifts from inconvenient to dangerous.
Frequent Flare-Ups (Exacerbations)
Exacerbations are sudden worsening episodes, usually triggered by infection or pollution. At Stage 3, these happen multiple times per year. Each one causes additional permanent lung damage. Hospital admissions become common.
Reduced Exercise Tolerance
Getting dressed causes breathlessness in some patients. Many stop leaving home. Skeletal muscles also weaken from inactivity and chronic systemic inflammation.
Oxygen Levels and Fatigue
Oxygen saturation starts dropping at rest in some Stage 3 patients. Chronic low oxygen causes headaches, confusion, and severe fatigue. Sleep quality drops because breathing is harder when lying flat.
Complications Begin to Develop
Cor pulmonale, where the right side of the heart enlarges from high lung pressure, develops in some Stage 3 patients. Pulmonary hypertension appears here, too. These are serious secondary conditions driven directly by COPD.
Stage 4 COPD: Advanced or End-Stage Disease
FEV1 drops below 30%. This is the endpoint of the 4 stages of COPD. Survival depends on how consistently symptoms are managed.
Very Severe Airflow Restriction
Breathing at rest requires effort. Short conversations cause breathlessness. Many patients need continuous oxygen support around the clock.
Chronic Respiratory Failure Risk
Carbon dioxide builds up when the lungs can’t expel it. This is hypercapnic respiratory failure. It causes drowsiness, confusion, and if untreated, unconsciousness. BiPAP machines manage this at home. Some patients eventually need mechanical ventilation.
Quality of Life Limitations
Independent living becomes difficult. Most patients need daily assistance. Depression rates in Stage 4 COPD exceed 40%, according to American Thoracic Society data.
Life Expectancy Considerations
Median survival after reaching Stage 4 is 2–5 years, depending on comorbidities and treatment adherence. Patients who stop smoking even at Stage 4 improve survival odds compared to those who continue.
Progression of Symptoms Across COPD Stages
The progression of symptoms across COPD stages is not uniform. Some patients stay at Stage 1 for decades. Others move from Stage 2 to Stage 4 in 5 years. The difference comes down to smoking status, exacerbation frequency, and genetic vulnerability.
Symptom Timeline from Mild to Severe
- Stage 1: Occasional cough, minimal breathlessness
- Stage 2: Exertional breathlessness, daily cough, mucus
- Stage 3: Breathlessness on minimal activity, frequent flare-ups
- Stage 4: Breathlessness at rest, low oxygen, respiratory failure risk
Why Progression Speed Varies
Heavy smokers who continue after diagnosis progress 3x faster than those who quit, based on GOLD cohort data. Frequent exacerbations add 30–40 ml of FEV1 loss per year beyond the baseline rate.
Role of Exacerbations in Disease Worsening
Each moderate-to-severe exacerbation leaves permanent damage. After 3 or more hospitalizations for COPD, 5-year survival drops below 50%. Preventing exacerbations is a core treatment goal from Stage 2 onward.
Treatment Options by COPD Stage
Treatment options by COPD stage change significantly as the disease progresses.
Stage-Wise Medication Approach
- Stage 1: Short-acting bronchodilator (SABA) as needed
- Stage 2: Long-acting bronchodilator (LABA or LAMA) daily
- Stage 3: LABA + LAMA combination; add ICS (inhaled corticosteroid) if frequent flare-ups
- Stage 4: Triple therapy (LABA + LAMA + ICS) plus supplemental oxygen if SpO2 falls below 88%
Bronchodilators and Inhaled Steroids
Bronchodilators open narrowed airways. They don’t fix lung damage but make breathing easier. Inhaled corticosteroids reduce inflammation. They’re not for everyone. Patients with eosinophil counts above 300 cells per µL and frequent exacerbations benefit most.
Oxygen Therapy in Advanced Stages
Long-term oxygen therapy (LTOT) is prescribed when resting SpO2 stays at or below 88%. It extends survival in Stage 4. The standard is 15 or more hours daily. Fewer hours have no proven survival benefit.
Pulmonary Rehabilitation Role
Pulmonary rehab combines exercise training with education. It works at every stage but delivers the most impact at Stages 2 and 3. A 2022 Cochrane review confirmed it reduces hospital admissions by 38% in COPD patients.
Surgical Options in Severe COPD
Lung volume reduction surgery (LVRS) removes the most damaged lung tissue, letting healthier sections expand. It works best for upper-lobe emphysema. Bronchoscopic lung volume reduction using endobronchial valves is a less invasive option for eligible Stage 3–4 patients.
Genetic Factors Affecting COPD Progression
Genetic factors affecting COPD progression are consistently underdiagnosed in clinical practice.
Alpha-1 Antitrypsin Deficiency Explained
Alpha-1 antitrypsin (AAT) is a protein that protects lung tissue from inflammation damage. People with AAT deficiency lack enough of it. Their lungs break down faster. COPD develops in their 40s, not their 60s.
Why Non-Smokers Can Develop COPD
About 25% of COPD cases are in non-smokers. AAT deficiency, childhood lung damage, sustained air pollution, and biomass fuel exposure (common in South Asia and Sub-Saharan Africa) all cause COPD without a single cigarette.
Who Should Get Genetic Testing
GOLD guidelines recommend AAT testing for all COPD patients at least once. It matters most for patients under 45, those without significant smoking history, or anyone with a family member diagnosed with early-onset COPD.
What Triggers Faster COPD Progression
- Continued smoking: The single biggest accelerant. Each pack-year adds measurable FEV1 decline.
- Air pollution: PM2.5 particulate matter triggers airway inflammation comparable to tobacco smoke.
- Recurrent infections: Bacterial infections like Haemophilus influenzae damage airway walls repeatedly with each episode.
- Poor inhaler technique: Up to 60% of patients use inhalers incorrectly, reducing drug delivery to near zero.
- Skipping medication: Missing LABA or LAMA doses allows chronic inflammation to continue without interruption.
When to Seek Medical Help in COPD
Sudden worsening breathlessness, bluish lips, or blue fingernails need emergency attention immediately. Blue coloring means blood oxygen has dropped to dangerous levels. This is not a “wait and see” situation.
See your doctor if:
- Your usual inhaler stops providing relief
- You have a cough with green or yellow mucus lasting more than 3 days
- Ankle swelling appears, which signals possible right heart strain
- You wake up gasping or with morning headaches
- Any activity now causes breathlessness that previously did not
Frequently Asked Questions
What are the 4 stages of COPD exactly?
The 4 stages of COPD are defined by FEV1 percentage: Stage 1 above 80%, Stage 2 at 50–79%, Stage 3 at 30–49%, Stage 4 below 30%. Stage 4 is end-stage disease with chronic respiratory failure risk and severely limited daily function.
How fast does COPD progress?
In active smokers, FEV1 declines 60–80 ml per year. People who quit drop back to 20–30 ml per year. Frequent exacerbations add 30–40 ml more annually on top of baseline decline. Progression speed is not fixed across patients.
Which stage of COPD is the most dangerous?
Stage 4. FEV1 is below 30%, chronic respiratory failure is a constant risk, and 5-year survival falls below 50% in most published studies. Each hospitalization at this stage worsens the long-term prognosis.
Can COPD stay mild for life?
Yes. Patients who quit smoking at Stage 1 and eliminate further irritant exposure sometimes maintain stable FEV1 for 10–15 years. Staying exacerbation-free is the strongest predictor of long-term stability at mild stages.
How is COPD diagnosed and staged?
Spirometry confirms diagnosis when FEV1/FVC falls below 0.70 post-bronchodilator. FEV1 percentage then determines the stage. Chest CT scans provide additional detail on emphysema extent and airway wall thickening.
What is the life expectancy with COPD?
Stage 1 and 2 patients have near-normal life expectancy if they quit smoking promptly. Stage 3 median survival is 8–10 years post-diagnosis. Stage 4 median survival is 2–5 years, varying significantly based on comorbidities and adherence.
Can non-smokers get COPD?
Yes. AAT deficiency, long-term biomass fuel exposure, severe childhood lung infections, and occupational dust cause COPD in non-smokers. Roughly 1 in 4 COPD patients never smoked at all.
When is oxygen therapy required?
Oxygen therapy starts when resting blood oxygen saturation confirms 88% or below on two separate readings taken 3 weeks apart during a stable period. Using it for 15 or more hours daily is the proven survival threshold.
What lifestyle changes help slow COPD?
Quitting smoking is the only lifestyle change with strong clinical evidence for slowing FEV1 decline. Annual flu vaccination and pneumococcal vaccination reduce exacerbation frequency. Pulmonary rehab cuts hospital admissions by 38%, per Cochrane data.
Is COPD considered a terminal illness?
Yes, COPD is incurable and progressive. But Stage 2 and 3 patients routinely live 15–20 more years with consistent management. Stage 4 is life-limiting, but survival varies widely based on treatment adherence and comorbidity control.











