

A period is considered late when it has not arrived within seven days past the expected date. Missing a period completely for six or more weeks from the start of the last one is classified as a missed period. In the United States, menstrual irregularities affect up to 14 to 25% of people with reproductive cycles at any given time. Most single delays are not medically serious, but repeated missed periods always require evaluation.
How late a period can be varies between individuals because menstrual cycles are not perfectly identical month to month. A healthy cycle can range from 21 to 35 days, and individual cycles can vary by up to seven days without indicating a disorder. Stress, weight changes, hormonal imbalance , and underlying conditions all delay periods through different biological mechanisms.
What Is Considered a Normal Menstrual Cycle?
A normal menstrual cycle runs from the first day of one period to the first day of the next. The average is 28 days, but a healthy range spans 21 to 35 days. Periods lasting two to seven days with a total blood loss of 20 to 80 milliliters are within normal parameters. Cycles shorter than 21 days or longer than 35 days consistently are considered irregular.
Average Cycle Length Explained
The menstrual cycle operates through four phases: menstruation, the follicular phase, ovulation, and the luteal phase. Ovulation (the release of an egg from the ovary) typically occurs around day 14 in a 28-day cycle, but it can shift to day 10 or day 20 depending on hormonal signals.
The luteal phase (time between ovulation and the start of the next period) is relatively fixed at 12 to 16 days. This means cycle length varies mostly based on when ovulation occurs, not how long the period lasts.
Natural Variation Between Individuals
No two people have identical cycle timing. Cycle length can shift by up to seven days from one month to the next in a healthy, regularly cycling person. Teenagers and people approaching perimenopause (the transitional phase before menopause, usually beginning in the mid-to-late 40s) show the most variation. Tracking at least three consecutive cycles gives a more accurate baseline than relying on a single month.
Irregular Periods vs. Occasional Delays
An occasional delay is a single late or missed period with no recurring pattern. Irregular periods are a persistent pattern of cycles shorter than 21 days, longer than 35 days, or unpredictably variable over multiple consecutive months.
Secondary amenorrhea (the medical term for missing three or more consecutive periods in someone who previously had them) always warrants clinical investigation.
How Many Days Late Can a Period Be?
A delay of one to five days is common and often caused by minor hormonal fluctuations. A delay of six to nine days warrants monitoring, especially if pregnancy is possible. A delay of ten or more days consistently points toward a specific cause and should be investigated, including testing for pregnancy if there is any chance of conception.
Short Delays That May Be Normal
A period that arrives one to seven days later than your tracked average is within the normal range of cycle variation for most people. Factors like a stressful week, a change in sleep schedule, a recent illness, or a change in diet can shift ovulation timing by several days and push the period back accordingly.
When a Missed Period Becomes Significant
A period that has not arrived 35 or more days from the start of the last one is medically considered a missed period, even if your cycle is usually shorter. Two or more consecutive missed periods without a clear temporary cause (like a known stressful event or recent travel) require evaluation. Take a home pregnancy test if your period is seven or more days late and you have had recent sexual contact.
Tracking Cycle Timing Accurately
Tracking your period requires recording the first day of bleeding each month, not the last. Many people mistakenly count from the last day, which produces inaccurate calculations.
Period tracking apps like Clue or Flo can identify your personal average cycle length after three months of consistent use. This personalized baseline is more useful than the textbook average of 28 days.
Stress Causing Delayed Periods
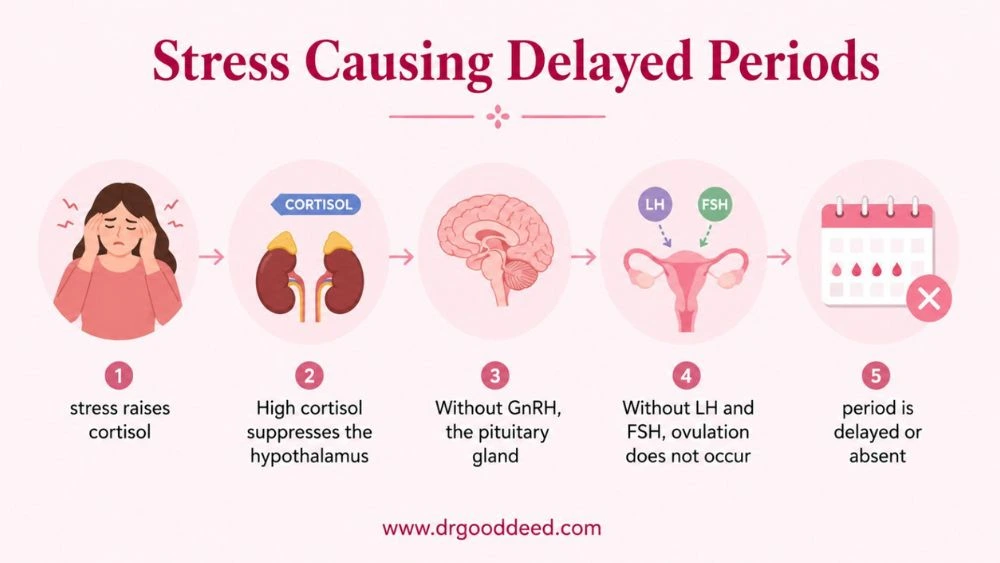
Stress-causing delayed periods is one of the most clinically well-documented connections in gynecology. High stress activates the hypothalamus (a region of the brain that controls hormone release). The hypothalamus responds to stress by suppressing GnRH (gonadotropin-releasing hormone), the signal that starts the hormonal chain leading to ovulation. No ovulation means no progesterone surge and no period.
How stress delays menstruation:
- Physical or emotional stress raises cortisol (stress hormone) levels
- High cortisol suppresses the hypothalamus from releasing GnRH
- Without GnRH, the pituitary gland (at the base of the brain) does not release LH (luteinizing hormone) and FSH (follicle-stimulating hormone)
- Without LH and FSH, ovulation does not occur
- Without ovulation, the luteal phase does not begin, and the period is delayed or absent
Stress-causing delayed periods can produce delays of one to four weeks in moderate cases. In severe or prolonged stress (trauma, grief, major illness, extreme work pressure), it can suppress periods for multiple months, a condition called stress-induced hypothalamic amenorrhea.
Weight Changes Affecting Menstruation
Weight changes affecting menstruation operate through the same hypothalamic pathway as stress. The body treats both rapid weight loss and excessive exercise as survival threats, suppressing reproduction to conserve energy.
Rapid Weight Loss and Missed Periods
Dropping body fat below a certain threshold, typically a BMI (Body Mass Index) below 18.5, disrupts the production of leptin (a hormone produced by fat cells that signals adequate energy to the brain).
Low leptin tells the hypothalamus to suppress GnRH and halt ovulation. Periods may stop within one to two months of reaching critically low body fat. This is one mechanism behind the menstrual disruption seen in eating disorders like anorexia nervosa.
Excessive Exercise and Hormonal Imbalance
The female athlete triad is a well-recognized clinical syndrome involving low energy availability (burning significantly more calories than consumed), menstrual dysfunction (ranging from irregular periods to complete absence), and low bone density.
Athletes in gymnastics, long-distance running, ballet, and cycling are at highest risk. A period that stops during intense training is not a sign of fitness. It indicates the body is diverting energy away from reproductive function.
Weight Gain and Irregular Ovulation
Significant weight gain disrupts menstruation through a different mechanism. Excess body fat increases estrogen production (fat cells convert androgens to estrogen), creating a chronic estrogen excess that interferes with the normal hormonal cycling required for ovulation.
This is one reason why PCOS (polycystic ovary syndrome, the most common hormonal disorder in reproductive-age women) is closely associated with higher body weight. Weight changes affecting menstruation in either direction ultimately affect ovulation timing, which determines when the period arrives.
PMS Symptoms With Late Period
PMS symptoms with late period are common and cause significant confusion. PMS (premenstrual syndrome) is driven by the hormonal changes of the luteal phase, not by the arrival of bleeding itself.
If ovulation is delayed, the entire luteal phase shifts later, including all PMS symptoms. You can experience bloating, breast tenderness, mood changes, cramps, and fatigue without the period arriving on the expected day.
Common PMS symptoms with late period scenarios:
- Ovulation occurred later than usual, pushing all subsequent hormone shifts back by one to two weeks
- The luteal phase is progressing normally but took longer to start due to delayed ovulation from stress or a weight change
- PMS symptoms plus a missed period alongside nausea, light spotting, or breast changes may indicate early pregnancy
PMS symptoms with late period do not confirm the period is coming. They indicate that the hormonal cycle is active but shifted. A pregnancy test is the only way to confirm or rule out pregnancy when symptoms appear but bleeding does not.
Could a Late Period Mean Pregnancy?
Pregnancy is the first cause to rule out when a period is seven or more days late and sexual activity has occurred. Without medical intervention, periods do not return until after delivery or pregnancy loss.
Early Pregnancy Symptoms
Early pregnancy symptoms appear within the first two to four weeks after conception and include:
- Breast tenderness or fullness
- Fatigue that feels unusually heavy
- Nausea (with or without vomiting), strongest in the morning but can occur at any time
- Mild pelvic cramping without bleeding
- Increased urination frequency
- Food aversions or heightened sense of smell
These symptoms overlap significantly with late-phase PMS, which is why a test is more reliable than symptom assessment alone.
Implantation Bleeding vs. Missed Periods
Implantation bleeding occurs when a fertilized egg attaches to the uterine wall, typically 10 to 14 days after conception. It is lighter than a normal period, usually appears as pink or brown spotting, lasts one to three days, and does not involve clots.
Many people mistake implantation bleeding for an early period. If bleeding is lighter than usual and stops sooner than a normal period, take a home pregnancy test.
When Pregnancy Testing May Help
Home urine pregnancy tests detect hCG (human chorionic gonadotropin, the pregnancy hormone). hCG reaches detectable levels in urine on or after the first day of a missed period for most tests. Testing before this date can produce false negatives. Testing on the first day of a missed period with a sensitive test (25 mIU/mL threshold) is accurate for most people. A negative result with ongoing missed periods requires a repeat test in one week or a blood test at a clinic.
Other Common Causes of Delayed Periods
Beyond pregnancy, stress, and weight changes, several medical conditions regularly delay periods.
Other causes of late or missed periods:
- PCOS (polycystic ovary syndrome): the most common hormonal cause of irregular cycles. PCOS disrupts ovulation through elevated androgens (male hormones) and insulin resistance, producing cycles that can extend to 45 to 90 days or stop entirely
- Thyroid dysfunction: both hypothyroidism (underactive thyroid) and hyperthyroidism (overactive thyroid) alter the hormonal environment needed for regular ovulation. A simple TSH blood test screens for both.
- Hyperprolactinemia: elevated prolactin levels (from a small benign pituitary tumor called a prolactinoma, or from certain medications) suppress ovulation
- Perimenopause: cycle irregularity begins four to eight years before menopause, which has a median US onset age of 51
- Certain medications: antipsychotics, antidepressants, chemotherapy agents, and high-dose corticosteroids can suppress menstruation
- Chronic illness: celiac disease, inflammatory bowel disease, and uncontrolled type 1 diabetes all affect menstrual regularity through systemic hormonal effects
How to Regulate Irregular Periods
Ways to regulate irregular periods depend entirely on the cause. There is no single solution because the mechanisms differ between PCOS, stress, weight-related amenorrhea, and thyroid conditions.
Approaches used to regulate irregular periods by cause:
- Stress-related delay: reducing cortisol through sleep improvement, reduced caffeine, mindfulness, and workload adjustment allows the hypothalamus to resume normal GnRH pulsing. Periods typically return within one to three months of addressing the stress source.
- Weight-related amenorrhea: restoring body weight or reducing training load by 10 to 20% allows leptin signaling to recover. Periods often return within two to four months, though bone density recovery takes longer.
- PCOS: low-glycemic diet, regular moderate exercise, and weight management reduce insulin resistance and improve ovulation frequency. Medications like metformin (which improves insulin sensitivity) or combined oral contraceptives are common medical approaches.
- Thyroid-related: thyroid hormone replacement (levothyroxine for hypothyroidism) or thyroid-suppressing medications restore cycle regularity in most cases within three to six months.
Lifestyle Habits That Affect Menstrual Cycles
Poor Sleep and Fatigue
The sleep-wake cycle regulates melatonin, which directly affects GnRH pulsing from the hypothalamus. Consistently sleeping fewer than six hours per night disrupts the hormonal rhythm that drives ovulation.
Understanding how late a period can be due to sleep issues matters because shift workers and people with irregular sleep schedules show significantly higher rates of menstrual irregularity than those with stable sleep patterns.
High Stress and Emotional Health
Acute stress (a difficult week or exam period) delays a single period. Chronic stress (ongoing financial pressure, relationship conflict, caregiving demands) can suppress ovulation for months.
The hypothalamic suppression from chronic stress is indistinguishable from the suppression caused by weight loss or overexercise. All three produce the same hormonal outcome through the same pathway.
Nutritional Deficiencies and Hydration
Deficiencies in iron, vitamin D, magnesium, and zinc have documented associations with menstrual irregularity. Vitamin D deficiency disrupts follicular development enough to delay ovulation by one to two weeks.
Iron deficiency does not directly delay periods but causes heavier bleeding that compounds anemia. Magnesium supports progesterone production in the luteal phase. Staying well-hydrated supports overall hormonal transport and reduces cramping intensity.
FAQs
How Many Days Late Can a Period Be Before Pregnancy Is Possible?
You cannot rule it out based on timing alone. A period that is seven or more days late with any chance of conception warrants a pregnancy test. Home tests are 99% accurate when taken on the first day of a missed period. A negative result followed by continued absence requires a repeat test in one week.
Can Stress Alone Delay Menstruation Significantly?
Yes. Stress-causing delayed periods works through cortisol suppression of the hypothalamus, which halts GnRH release and delays or prevents ovulation. A single acutely stressful event (a move, a breakup, a major exam) can delay a period by one to four weeks. Chronic stress can suppress periods for two to six months without any other contributing factor.
Why Do PMS Symptoms Sometimes Happen Without a Period Starting?
PMS symptoms with late period happen because PMS is triggered by the luteal phase hormones (progesterone drop and estrogen fluctuation), not by bleeding itself. If ovulation was delayed by two weeks, PMS symptoms appear two weeks later than usual. The period eventually arrives, but the symptom-to-period gap extends. If PMS symptoms appear alongside nausea or missed bleeding, test for pregnancy.
How Do Weight Changes Affect Ovulation and Menstrual Cycles?
Weight changes affecting menstruation disrupt the leptin-hypothalamus communication. Rapid weight loss below BMI 18.5 reduces leptin enough to suppress GnRH and halt ovulation. Weight gain above a certain threshold increases estrogen from fat cells, interfering with the LH surge needed for ovulation. Both extremes delay or stop periods through separate mechanisms.
Can Excessive Exercise Lead to Missed Periods?
Yes. The female athlete triad links high training volume with menstrual loss when caloric intake does not match energy expenditure. Periods stop when energy deficiency signals the hypothalamus to suppress reproduction. Reducing training intensity by 10 to 20% and increasing caloric intake typically restores menstruation within two to four months. It can be absent for months to years without treatment.
When Should Pregnancy Testing Be Considered After a Missed Period?
Test on the first day of a missed period if sexual activity has occurred. A first-morning urine sample produces the most concentrated hCG and the most reliable result. A negative test with continuing absent periods should be repeated in seven days. If two tests are negative and the period remains absent for three or more weeks past its expected date, see a healthcare provider for a blood hCG test and hormonal evaluation.
Are Irregular Cycles Common During Hormonal Changes or Perimenopause?
Yes. Perimenopause, which begins an average of four to eight years before menopause (typically in the mid-40s), produces significant cycle variability. Cycles may shorten to 21 days, lengthen to 45 days, or become unpredictable within the same year. FSH (follicle-stimulating hormone) rises as ovarian reserve declines, disrupting the consistent hormonal pattern needed for regular cycles. Pregnancy remains possible during perimenopause until menopause is confirmed.
What Medical Conditions Commonly Cause Delayed Periods?
PCOS is the most common, affecting 8 to 13% of reproductive-age women in the US. Hypothyroidism causes menstrual delay in 20 to 30% of affected women. Hyperprolactinemia from a prolactinoma suppresses ovulation in proportion to prolactin levels. Premature ovarian insufficiency (POI), where ovarian function declines before age 40, causes irregular then absent periods in 1% of women.
How Can Menstrual Cycles Be Tracked More Accurately?
Record the first day of bleeding each month, not the last. Track for at least three consecutive cycles before identifying your personal average. Note any factors like high-stress weeks, illness, travel, or significant diet changes alongside cycle dates. Apps like Clue, Flo, or Natural Cycles use basal body temperature and symptom data to improve prediction accuracy beyond simple calendar counting.
When Should Repeated Missed Periods Be Medically Evaluated?
See a healthcare provider if you have missed two or more consecutive periods without a confirmed cause, if how late can a period be in your case has exceeded six weeks repeatedly, or if periods have been absent for three or more months (secondary amenorrhea). Evaluation typically includes blood tests for FSH, LH, prolactin, TSH, testosterone, and hCG, along with a pelvic ultrasound to assess ovarian structure.











1 Comment
Comments are closed.