Strokes and diabetes share a direct biological connection. Adults with type 2 diabetes face 1.5 to 3 times the stroke risk of people without diabetes, according to data from the American Diabetes Association. High blood glucose damages artery walls, promotes clot formation, and accelerates atherosclerosis simultaneously. These three processes happen together, quietly, often years before a stroke occurs.
How Diabetes Increases Stroke Risk
Diabetes increases stroke risk and involves three overlapping processes: vessel wall damage, arterial narrowing, and increased blood clotting. Together they create the biological conditions for both ischemic and hemorrhagic stroke. Unlike most single-cause risk factors, diabetes attacks the circulatory system on multiple fronts at the same time.
High Glucose Damaging Blood Vessels
High glucose damaging blood vessels begins with a chemical process called glycation. Excess glucose in the bloodstream attaches to proteins inside artery walls, forming compounds called advanced glycation end-products (AGEs). AGEs stiffen and weaken vessel walls, making them vulnerable to cracking under normal blood pressure. This damage builds over years of elevated blood sugar.
Thickening and Narrowing of Arteries
Chronic high blood glucose triggers inflammation inside arteries. Inflammatory cells accumulate, fatty deposits build up, and artery walls thicken progressively. The opening inside the artery narrows. Less blood flows through. Brain regions that depend on small arteries, which diabetics damage faster than non-diabetics, become starved of oxygen.
Increased Clot Formation and Reduced Blood Flow
Diabetes makes platelets hyperactive. Platelets are the blood cells responsible for clotting. In diabetics, they stick together more easily and form clots with less trigger than in non-diabetics. At the same time, the damaged inner artery lining loses its natural ability to prevent clots from forming. Both effects push simultaneously toward blockage.
High Glucose Damaging Blood Vessels
High glucose damaging blood vessels is the root cause connecting strokes and diabetes. It operates at the microscopic level inside the vessel wall itself, which is why blood sugar control is more than a diabetes management issue. It is stroke prevention.
Endothelial Damage (Inner Vessel Lining)
The inner lining of every blood vessel, called the endothelium, normally produces nitric oxide. Nitric oxide keeps blood vessels relaxed and open. High blood glucose reduces nitric oxide production. Without it, vessels constrict, blood pressure rises inside them, and the lining becomes prone to micro-tears. Each micro-tear is a site where a clot can form.
Atherosclerosis Progression
Diabetics develop atherosclerosis, the buildup of plaques inside arteries, about 10 to 15 years earlier than non-diabetics. The carotid arteries in the neck, which carry blood directly to the brain, are among the first affected. When a carotid plaque ruptures, it sends debris directly into the brain’s blood supply. That is an ischemic stroke.
Reduced Oxygen Supply to Brain
Narrowed, stiff arteries carry less blood per heartbeat. Over time, specific brain regions receive chronically reduced oxygen. This is the mechanism behind silent strokes, which are small brain injuries with no dramatic symptoms. Studies show that diabetics suffer silent strokes at significantly higher rates than the general population, and these accumulate into measurable cognitive decline.
Stroke Symptoms in Diabetic Patients
Stroke symptoms in diabetic patients are sometimes missed or misread, and that delay costs brain tissue. Every minute of stroke, approximately 1.9 million neurons die, according to the American Stroke Association. Two factors in diabetes make symptom recognition harder: diabetic neuropathy dulls sensation, and hypoglycemia low blood sugar mimics stroke with similar confusion and weakness.
Sudden Weakness or Numbness
In non-diabetics, sudden arm or leg weakness signals an emergency immediately. In diabetics with peripheral neuropathy, baseline numbness and weakness already exist. A new or worsening one-sided weakness can get dismissed as a “bad nerve day.” It usually isn’t.
Difficulty Speaking or Understanding
Sudden slurred speech or inability to form words points to the left hemisphere of the brain losing blood supply. This symptom has no diabetic mimic. When it appears, call 911 immediately.
Vision Problems
Sudden blurred vision or vision loss in one eye points to interrupted blood flow to the retina or visual cortex. Diabetic retinopathy already affects vision in many diabetics, but retinopathy changes happen gradually. Sudden vision loss is not retinopathy.
Loss of Balance
Sudden inability to stand, walk, or coordinate movements without another obvious cause points to the cerebellum or brainstem losing blood flow. Diabetics sometimes attribute balance problems to blood sugar fluctuation. A balance problem that comes on in seconds is not a glucose issue.
Sudden Numbness Diabetic Stroke Signs
Sudden numbness diabetic stroke signs are the most frequently missed warning indicators in people living with diabetes. The critical word is “sudden.” Diabetic neuropathy causes gradual, symmetric numbness, usually in the feet and legs. Stroke causes sudden, one-sided numbness anywhere in the body.
One-Sided Body Numbness
Numbness affecting only the left arm, only the right leg, or only one side of the face appeared in seconds is a stroke sign. Diabetic neuropathy doesn’t work that way. It builds slowly and affects both sides. Sudden numbness diabetic stroke signs always arrive without warning.
Facial Drooping
One side of the face dropping when trying to smile is the most visible and recognizable sign. Ask the person to show their teeth. If one side doesn’t move, that is stroke until proven otherwise.
Arm or Leg Weakness
Ask the person to raise both arms parallel to the ground and hold them there. If one arm drifts downward without the person trying to move it, that is called “pronator drift.” It indicates motor cortex disruption from stroke. This test takes five seconds and is clinically reliable.
Risk Factors That Increase Stroke in Diabetes
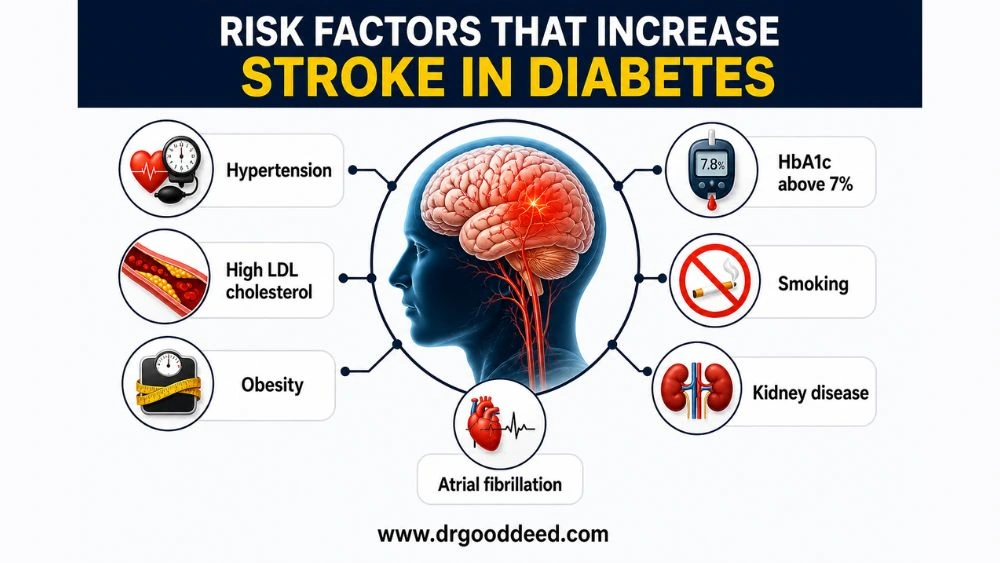
Diabetes alone raises stroke risk. These additional factors multiply it further. Diabetics in the US who carry two or more of these risk factors face compound vascular risk that goes well beyond the general population’s baseline.
- Hypertension: Present in about 70% of US adults with type 2 diabetes. High BP combined with diabetes damages arteries faster than either condition alone
- High LDL cholesterol: Fuels atherosclerotic plaque growth in carotid and cerebral arteries
- Obesity: Particularly central (abdominal) obesity promotes insulin resistance and systemic inflammation
- Atrial fibrillation: More common in diabetics; sends blood clots directly to the brain
- HbA1c above 7%: Each 1% rise in HbA1c correlates with measurably higher stroke risk in longitudinal studies
- Smoking: Doubles the rate of atherosclerosis progression in diabetics specifically
- Kidney disease (diabetic nephropathy): Signals advanced vascular damage across all organ systems, including the brain
Types of Stroke Common in Diabetic Patients
Strokes and diabetes don’t pair randomly. Specific stroke types occur at higher rates in diabetic populations because of the particular vessels that high blood sugar damages most aggressively.
Ischemic Stroke (Most Common)
Ischemic stroke accounts for about 87% of all strokes in the US, and the proportion is even higher in diabetics. A blood clot blocks an artery supplying the brain. In diabetics, hyperactive platelets and damaged artery walls create this scenario more often and at younger ages.
Lacunar Stroke (Small Vessel Disease)
Lacunar strokes occur in the brain’s tiny deep arteries. These small vessels are the first ones destroyed by chronic high blood glucose. Lacunar strokes are the most common stroke subtype specifically linked to diabetes and long-term hypertension. They often produce no dramatic symptoms but accumulate into serious disability over time.
Hemorrhagic Stroke (Less Common)
Hemorrhagic stroke occurs when a weakened brain artery ruptures. It is less common in diabetics than ischemic stroke but carries a higher death rate when it does occur. Brittle, AGE-damaged artery walls in poorly controlled diabetics raise hemorrhagic risk above the general population.
How to Prevent Stroke in Diabetes
Preventing strokes and diabetes complications requires targeting both blood sugar and vascular health at the same time. Blood sugar control alone is not sufficient.
- Keep HbA1c below 7% consistently; the UKPDS trial showed this reduces microvascular complications significantly
- Maintain blood pressure below 130/80 mmHg; this single target reduces stroke risk in diabetics by approximately 44%
- Take prescribed statins even with normal LDL; statin therapy reduces stroke risk by 25% in diabetics regardless of baseline cholesterol
- Eat a diet low in refined carbohydrates, processed meat, and sodium; the PREDIMED trial found a Mediterranean diet reduced cardiovascular events by 30% in high-risk individuals
- Exercise for at least 150 minutes weekly; aerobic activity lowers both blood glucose and blood pressure simultaneously
- Stop smoking; the stroke risk reduction from quitting begins within 12 months
- If atrial fibrillation is present, take anticoagulants as prescribed without skipping doses
- Check blood pressure at home daily and log readings alongside fasting glucose levels
FAQs
How are strokes and diabetes related?
Strokes and diabetes connect through three simultaneous processes: high glucose damages artery walls, thickened arteries reduce blood flow to the brain, and hyperactive platelets form clots more easily. Diabetics face 1.5 to 3 times the stroke risk of non-diabetics, with lacunar stroke being the most specifically linked type.
What are sudden numbness diabetic stroke signs?
Sudden numbness diabetic stroke signs are one-sided, appear within seconds, and affect the face, arm, or leg separately. Diabetic neuropathy causes gradual, bilateral foot and leg numbness. Stroke causes sudden, asymmetric numbness. The one-sided and sudden onset is the critical difference.
Can controlling diabetes prevent stroke?
Yes. Keeping HbA1c below 7% slows endothelial damage and atherosclerosis progression. Controlling blood pressure below 130/80 mmHg reduces stroke risk in diabetics by approximately 44%, based on the UK Prospective Diabetes Study. Blood sugar control alone without blood pressure control provides incomplete protection.
What type of stroke is common in diabetics?
Lacunar stroke, involving the brain’s small deep arteries, is the most specifically linked to diabetes. Ischemic stroke overall remains the most common type in diabetics (about 87% of cases). Lacunar strokes often cause no obvious acute symptoms, making them the most frequently missed stroke type in this group.
Why are stroke symptoms missed in diabetes?
Stroke symptoms in diabetic patients get missed because diabetic neuropathy already causes baseline numbness and weakness, making new one-sided deficits feel familiar. Hypoglycemia mimics stroke with confusion and slurred speech. Clinicians and patients both misread these overlapping symptoms. Sudden onset and one-sidedness are the distinguishing features.
What should diabetics do during a stroke emergency?
Call 911 immediately. Do not attempt to correct blood sugar first. Post-stroke hyperglycemia, where blood glucose rises during stroke, worsens brain injury independently. Emergency physicians must manage this. Do not eat, drink, or take medications while waiting. Note the exact time symptoms started; this determines IV tPA eligibility.
When should a diabetic patient see a doctor?
See a doctor immediately if any sudden one-sided symptom appears, including numbness, weakness, facial drooping, or speech difficulty. See a doctor within one week if HbA1c results exceed 7% or blood pressure readings consistently exceed 130/80 mmHg. Strokes and diabetes risk compounds fast when both are uncontrolled.